

Diagnosis trajectories of prior multi-morbidity predict sepsis mortality
- PMID: 27812043
- PMCID: PMC5095673
- DOI: 10.1038/srep36624
Diagnosis trajectories of prior multi-morbidity predict sepsis mortality
Abstract
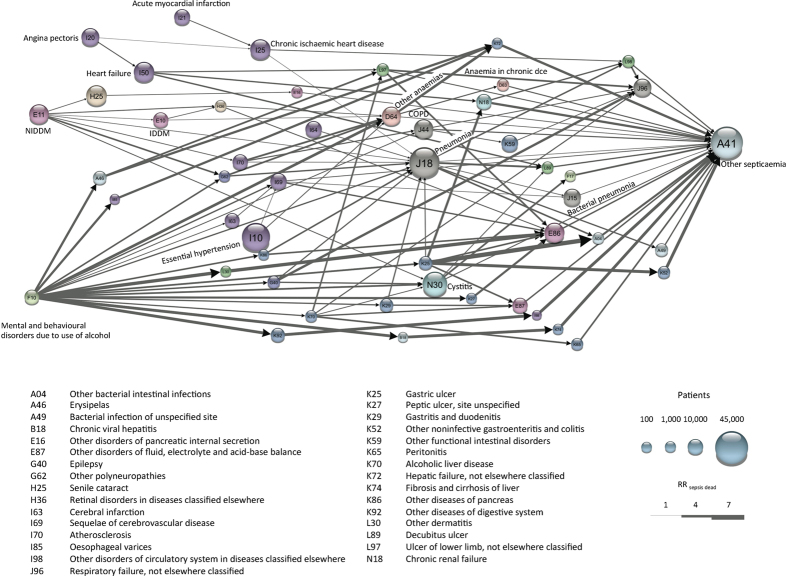
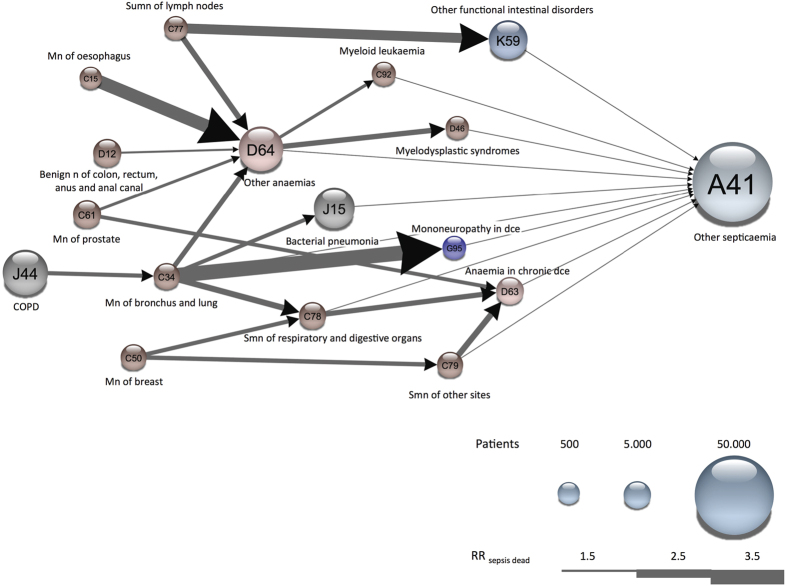
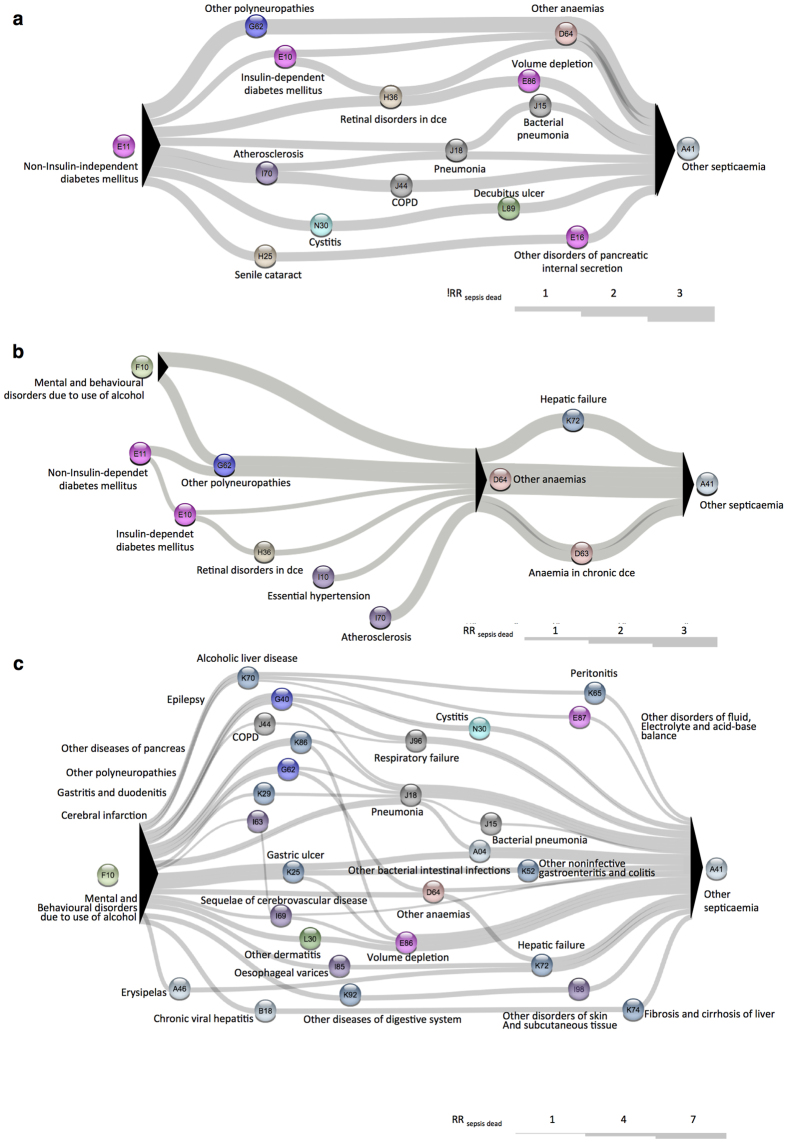
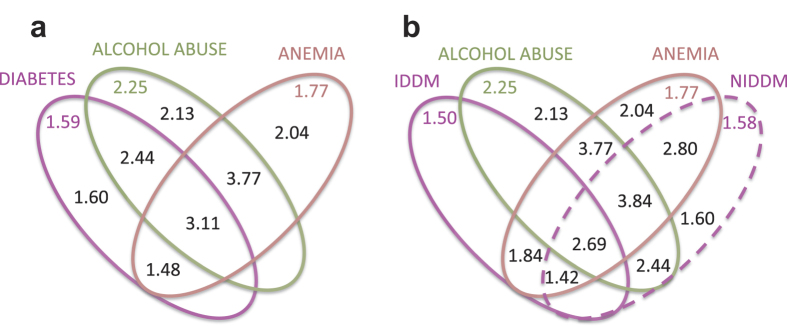
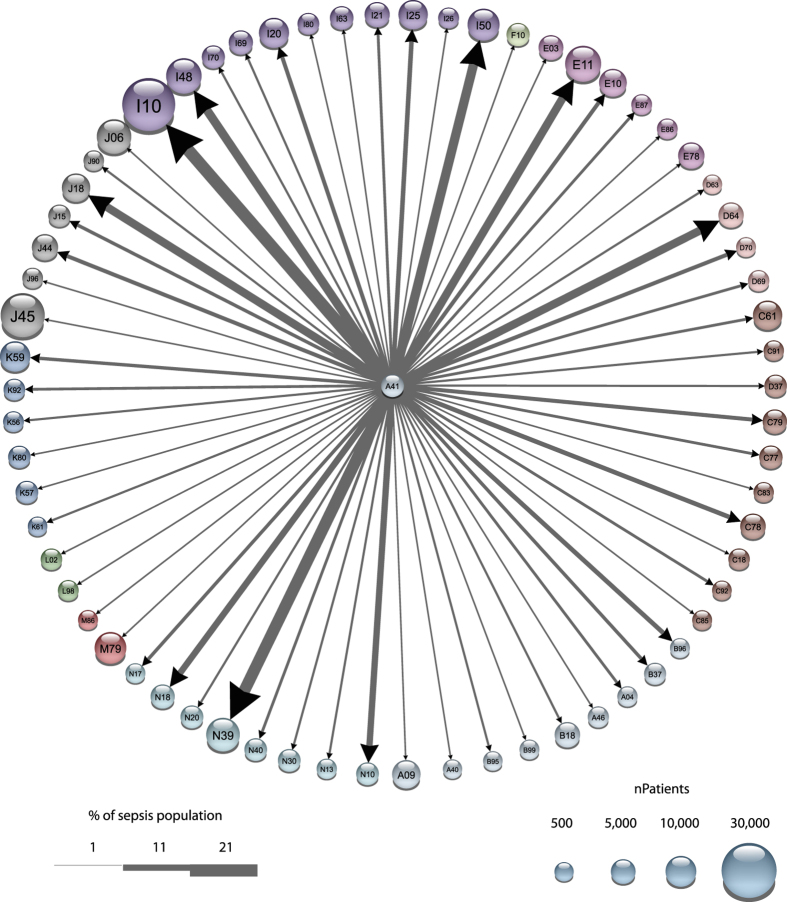
Sepsis affects millions of people every year, many of whom will die. In contrast to current survival prediction models for sepsis patients that primarily are based on data from within-admission clinical measurements (e.g. vital parameters and blood values), we aim for using the full disease history to predict sepsis mortality. We benefit from data in electronic medical records covering all hospital encounters in Denmark from 1996 to 2014. This data set included 6.6 million patients of whom almost 120,000 were diagnosed with the ICD-10 code: A41 'Other sepsis'. Interestingly, patients following recurrent trajectories of time-ordered co-morbidities had significantly increased sepsis mortality compared to those who did not follow a trajectory. We identified trajectories which significantly altered sepsis mortality, and found three major starting points in a combined temporal sepsis network: Alcohol abuse, Diabetes and Cardio-vascular diagnoses. Many cancers also increased sepsis mortality. Using the trajectory based stratification model we explain contradictory reports in relation to diabetes that recently have appeared in the literature. Finally, we compared the predictive power using 18.5 years of disease history to scoring based on within-admission clinical measurements emphasizing the value of long term data in novel patient scores that combine the two types of data.
Figures
References
-
- Lui V. et al.. Hospital Deaths in Patients With Sepsis From 2 Independent Cohorts. J. Am. Med. Assoc. 312, 90–92 (2014). - PubMed
-
- Gofton T. E. & Young G. B. Sepsis-associated encephalopathy. Nat. Rev. Neurol. 8, 557–566 (2012). - PubMed
-
- Steckert A. V., Alves de Castro A., Quevedo J. & Dal-Pizzol F. Sepsis in the Central Nervous System and Antioxidant Strategies with N-Acetylcysteine, Vitamins, and Statins. Curr. Neurovasc. Res. 11, 83–90 (2014). - PubMed
-
- Osias J. & Manno E. Neuromuscular complications of critical illness. Crit. Care Clin. 30, 785–794 (2014). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
