

A Comparative Study of Clinical Presentation and Risk Factors for Adverse Outcome in Patients Hospitalised with Acute Respiratory Disease Due to MERS Coronavirus or Other Causes
- PMID: 27812197
- PMCID: PMC5094725
- DOI: 10.1371/journal.pone.0165978
A Comparative Study of Clinical Presentation and Risk Factors for Adverse Outcome in Patients Hospitalised with Acute Respiratory Disease Due to MERS Coronavirus or Other Causes
Abstract
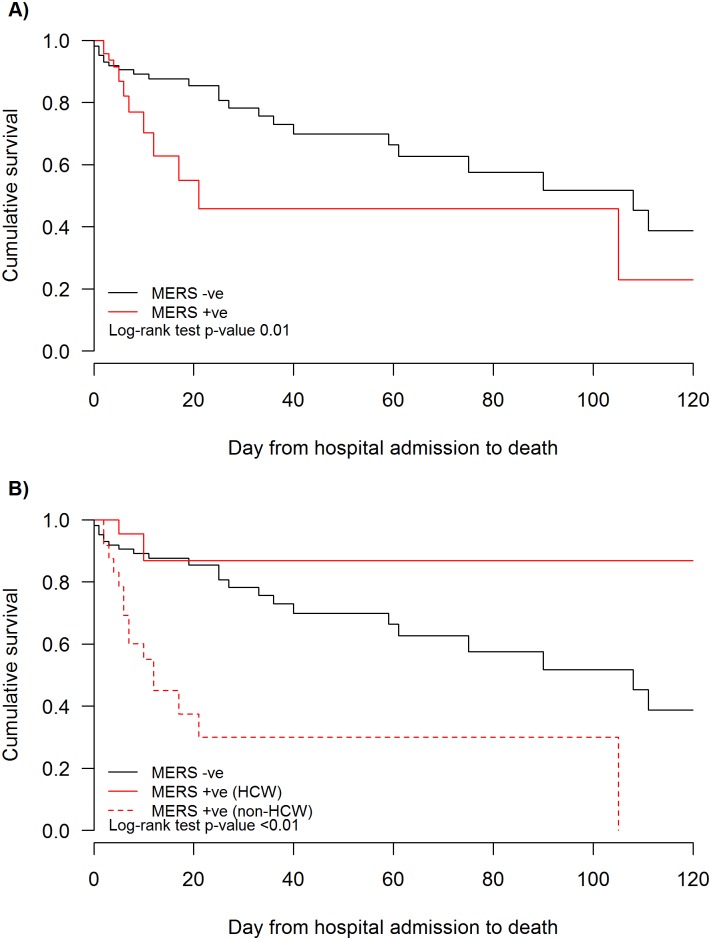
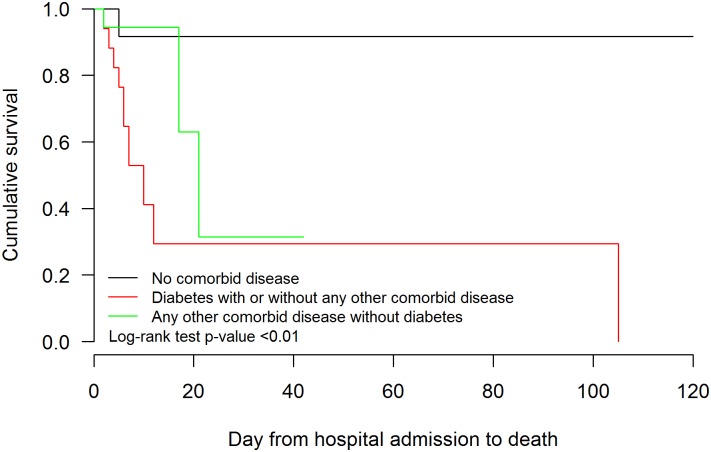
Middle East Respiratory syndrome (MERS) first emerged in Saudi Arabia in 2012 and remains a global health concern. The objective of this study was to compare the clinical features and risk factors for adverse outcome in patients with RT-PCR confirmed MERS and in those with acute respiratory disease who were MERS-CoV negative, presenting to the King Fahad Medical City (KFMC) in Riyadh between October 2012 and May 2014. The demographics, clinical and laboratory characteristics and clinical outcomes of patients with RT-PCR confirmed MERS-CoV infection was compared with those testing negative MERS-CoV PCR. Health care workers (HCW) with MERS were compared with MERS patients who were not health care workers. One hundred and fifty nine patients were eligible for inclusion. Forty eight tested positive for MERS CoV, 44 (92%) being hospital acquired infections and 23 were HCW. There were 111 MERS-CoV negative patients with acute respiratory illnesses included in this study as "negative controls". Patient with confirmed MERS-CoV infection were not clinically distinguishable from those with negative MERS-CoV RT-PCR results although diarrhoea was commoner in MERS patients. A high level of suspicion in initiating laboratory tests for MERS-CoV is therefore indicated. Variables associated with adverse outcome were older age and diabetes as a co-morbid illness. Interestingly, co-morbid illnesses other than diabetes were not significantly associated with poor outcome. Health care workers with MERS had a markedly better clinical outcome compared to non HCW MERS patients.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Clinical management of respiratory syndrome in patients hospitalized for suspected Middle East respiratory syndrome coronavirus infection in the Paris area from 2013 to 2016.BMC Infect Dis. 2018 Jul 16;18(1):331. doi: 10.1186/s12879-018-3223-5. BMC Infect Dis. 2018. PMID: 30012113 Free PMC article.
-
Occurrence of the Middle East Respiratory Syndrome Coronavirus (MERS-CoV) across the Gulf Corporation Council countries: Four years update.PLoS One. 2017 Oct 13;12(10):e0183850. doi: 10.1371/journal.pone.0183850. eCollection 2017. PLoS One. 2017. PMID: 29028812 Free PMC article.
-
Impact of Middle East Respiratory Syndrome coronavirus (MERS-CoV) on pregnancy and perinatal outcome.BMC Infect Dis. 2016 Mar 2;16:105. doi: 10.1186/s12879-016-1437-y. BMC Infect Dis. 2016. PMID: 26936356 Free PMC article.
-
[Etiological, epidemiological and clinical aspects of coronavirus infection MERS-CoV].Pol Merkur Lekarski. 2015 Jan;38(223):46-50. Pol Merkur Lekarski. 2015. PMID: 25763589 Review. Polish.
-
Severe acute respiratory syndrome vs. the Middle East respiratory syndrome.Curr Opin Pulm Med. 2014 May;20(3):233-41. doi: 10.1097/MCP.0000000000000046. Curr Opin Pulm Med. 2014. PMID: 24626235 Review.
Cited by
-
Mechanism of higher risk for COVID-19 in diabetes: a mask to lift.Endocrine. 2020 Sep;69(3):477-480. doi: 10.1007/s12020-020-02423-0. Epub 2020 Jul 23. Endocrine. 2020. PMID: 32705411 Free PMC article.
-
Multiple organ injury on admission predicts in-hospital mortality in patients with COVID-19.J Med Virol. 2021 Mar;93(3):1652-1664. doi: 10.1002/jmv.26534. Epub 2020 Sep 30. J Med Virol. 2021. PMID: 32949175 Free PMC article.
-
Comorbid diabetes results in immune dysregulation and enhanced disease severity following MERS-CoV infection.JCI Insight. 2019 Oct 17;4(20):e131774. doi: 10.1172/jci.insight.131774. JCI Insight. 2019. PMID: 31550243 Free PMC article.
-
Evaluation of visual triage for screening of Middle East respiratory syndrome coronavirus patients.New Microbes New Infect. 2018 Aug 11;26:49-52. doi: 10.1016/j.nmni.2018.08.008. eCollection 2018 Nov. New Microbes New Infect. 2018. PMID: 30224971 Free PMC article.
-
Prevention and management of COVID-19 among patients with diabetes: an appraisal of the literature.Diabetologia. 2020 Aug;63(8):1440-1452. doi: 10.1007/s00125-020-05164-x. Epub 2020 May 14. Diabetologia. 2020. PMID: 32405783 Free PMC article. Review.
References
-
- World Health Organization. Middle East Respiratory Syndrome coronavirus (MERS-CoV). Available: http://www.who.int/emergencies/mers-cov/en/. Accessed 2 August 2016.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
