

Knee donor-site morbidity after mosaicplasty - a systematic review
- PMID: 27813019
- PMCID: PMC5095115
- DOI: 10.1186/s40634-016-0066-0
Knee donor-site morbidity after mosaicplasty - a systematic review
Abstract
Background: Mosaicplasty has been associated with good short- to long-term results. Nevertheless, the osteochondral harvesting is restricted to the donor-site area available and it may lead to significant donor-site morbidity.
Purpose: Provide an overview of donor-site morbidity associated with harvesting of osteochondral plugs from the knee joint in mosaicplasty procedure.
Methods: Comprehensive search using Pubmed, Cochrane Library, SPORTDiscus and CINAHL databases was carried out through 10th October of 2016. As inclusion criteria, all English-language studies that assessed the knee donor-site morbidity after mosaicplasty were accepted. The outcomes were the description and rate of knee donor-site morbidity, sample's and cartilage defect's characterization and mosaicplasty-related features. Correlation between mosaicplasty features and rate of morbidity was performed. The methodological and reporting quality were assessed according to Coleman's methodology score.
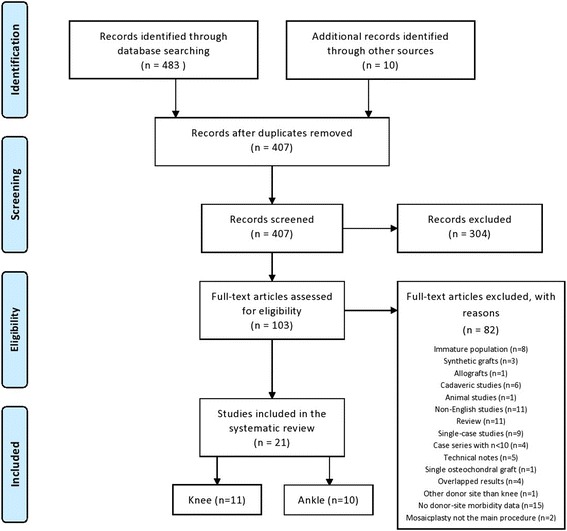
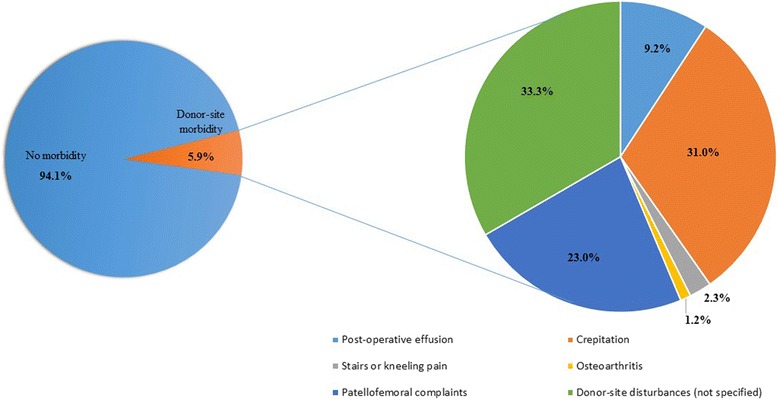
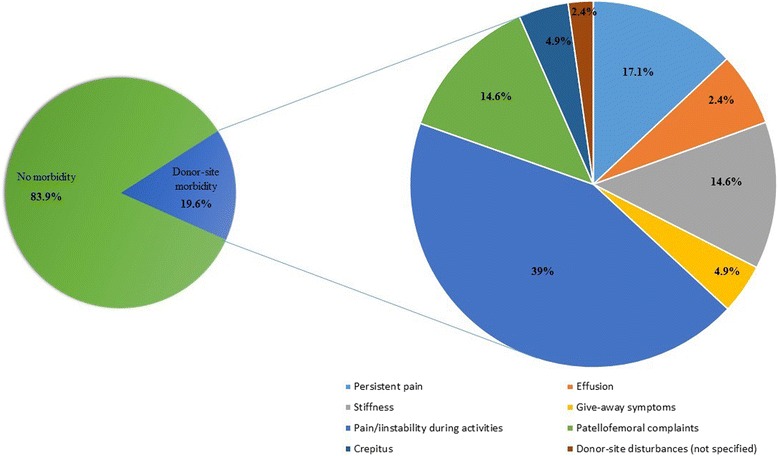
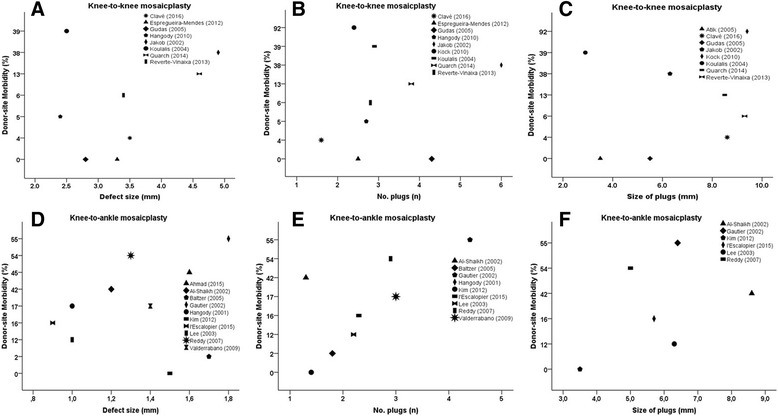
Results: Twenty-one studies were included, comprising a total of 1726 patients, with 1473 and 268 knee and ankle cartilage defects were included. The defect size ranged from 0.85 cm2 to 4.9 cm2 and most commonly 3 or less plugs (averaging 2.9 to 9.4 mm) were used. Donor-site for osteochondral harvesting included margins of the femoral trochlea (condyles), intercondylar notch, patellofemoral joint and upper tibio-fibular joint. Mean donor-site morbidity was 5.9 % and 19.6 % for knee and ankle mosaicplasty procedures, respectively. Concerning knee-to-knee mosaicplasty procedures, the most common donor-site morbidity complaints were patellofemoral disturbances (22 %) and crepitation (31 %), and in knee-to-ankle procedures there was a clear tendency for pain or instability during daily living or sports activities (44 %), followed by patellofemoral disturbances, knee stiffness and persistent pain (13 % each). There was no significant correlation between rate of donor-site morbidity and size of the defect, number and size of the plugs (p > 0.05).
Conclusions: Osteochondral harvesting in mosaicplasty often results in considerable donor-site morbidity. The donor-site morbidity for knee-to-ankle (16.9 %) was greater than knee-to-knee (5.9 %) mosaicplasty procedures, without any significant correlation between rate of donor-site morbidity and size of the defect, number and size of the plugs. Lack or imcomplete of donor-site morbidity reporting within the mosaicplasty studies is a concern that should be addressed in future studies.
Level of evidence: Level IV, systematic review of Level I-IV studies.
Keywords: Articular cartilage lesions; Donor-site morbidity; Knee; Mosaicplasty; Osteochondral.
Figures
References
-
- Ahmad J, Jones K (2015) Comparison of osteochondral autografts and allografts for treatment of recurrent or large talar osteochondral lesions. Foot Ankle Int. doi:10.1177/1071100715603191 - PubMed
-
- Al-Shaikh RA, Chou LB, Mann JA, Dreeben SM, Prieskorn D. Autologous osteochondral grafting for talar cartilage defects. Foot Ankle Int. 2002;23(5):381–389. - PubMed
-
- Atik OS, Uslu MM, Eksioglu F. Osteochondral multiple autograft transfer (OMAT) for the treatment of cartilage defects in the knee joint. Bull Hosp Jt Dis. 2005;63(1-2):37–40. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
