

Increased Proliferation of the Pancreatic Duct Gland Compartment in Type 1 Diabetes
- PMID: 27813705
- PMCID: PMC5413103
- DOI: 10.1210/jc.2016-3001
Increased Proliferation of the Pancreatic Duct Gland Compartment in Type 1 Diabetes
Abstract
Context: Pancreatic duct glands (PDGs) have been proposed as a source of regeneration in response to exocrine pancreas injury, and thus may serve as an organ stem cell niche. There is evidence to suggest ongoing β-cell formation in longstanding type 1 diabetes (T1D), but the source is unknown.
Objective: To investigate the PDG compartment of the pancreas in humans with T1D for evidence of an active regenerative signature (presence of progenitor cells and increased proliferation) and, in particular, as a potential source of β-cells.
Design, setting, and participants: Pancreases from 46 brain dead organ donors (22 with T1D, 24 nondiabetic controls) were investigated for activation (increased proliferation) and markers of pancreatic exocrine and endocrine progenitors.
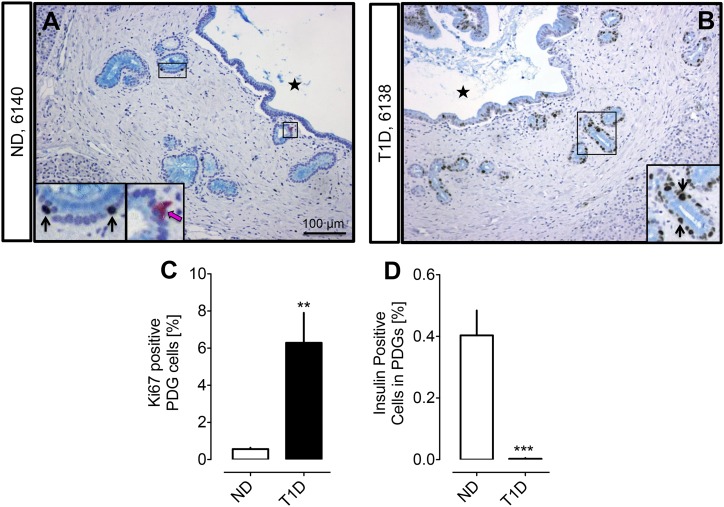
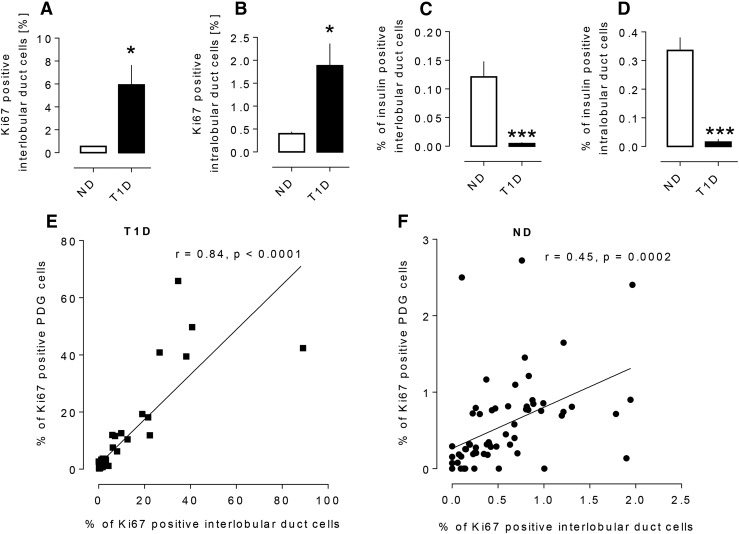
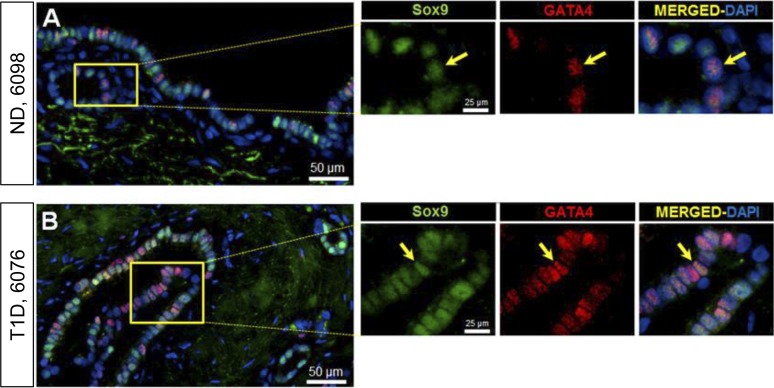
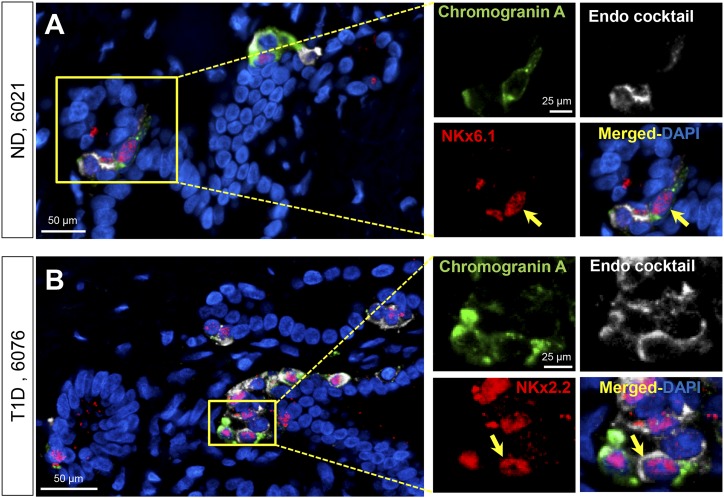
Results: PDG cell replication was increased in T1D (6.3% ± 1.6% vs 0.6% ± 0.1%, P < 0.001, T1D vs nondiabetic), most prominently in association with pancreatic inflammation. There were increased progenitor-like cells in PDGs of T1D, but predominantly with an exocrine fate.
Conclusion: The PDG compartment is activated in T1D consistent with a response to ongoing inflammation, and via resulting ductal hyperplasia may contribute to local obstructive pancreatitis and eventual pancreatic atrophy characteristic of T1D. However, there is no evidence of effective endocrine cell formation from PDGs.
Copyright © 2017 by the Endocrine Society
Figures
References
-
- Klöppel G, Löhr M, Habich K, Oberholzer M, Heitz PU. Islet pathology and the pathogenesis of type 1 and type 2 diabetes mellitus revisited. Surv Synth Pathol Res. 1985;4(2):110–125. - PubMed
-
- Meier JJ, Bhushan A, Butler AE, Rizza RA, Butler PC. Sustained beta cell apoptosis in patients with long-standing type 1 diabetes: indirect evidence for islet regeneration? Diabetologia. 2005;48(11):2221–2228. - PubMed
-
- Gepts W. Pathologic anatomy of the pancreas in juvenile diabetes mellitus. Diabetes. 1965;14(10):619–633. - PubMed
-
- Sjöberg S, Gunnarsson R, Gjötterberg M, Lefvert AK, Persson A, Ostman J. Residual insulin production, glycaemic control and prevalence of microvascular lesions and polyneuropathy in long-term type 1 (insulin-dependent) diabetes mellitus. Diabetologia. 1987;30(4):208–213. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
