

Impact of artifacts on VOR gain measures by video-oculography in the acute vestibular syndrome
- PMID: 27814312
- PMCID: PMC6054448
- DOI: 10.3233/VES-160587
Impact of artifacts on VOR gain measures by video-oculography in the acute vestibular syndrome
Abstract
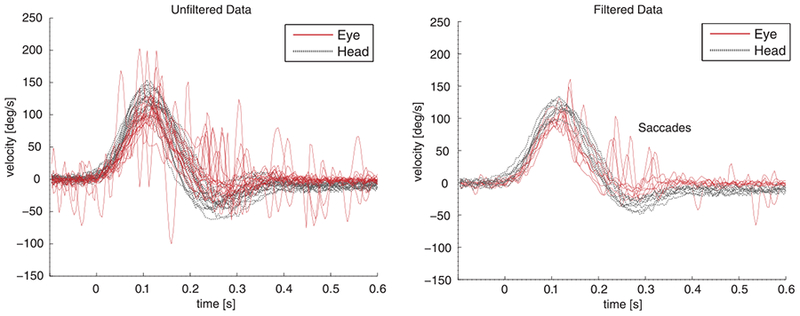
Objective: The video head impulse test (HIT) measures vestibular function (vestibulo-ocular reflex [VOR] gain - ratio of eye to head movement), and, in principle, could be used to make a distinction between central and peripheral causes of vertigo. However, VOG recordings contain artifacts, so using unfiltered device data might bias the final diagnosis, limiting application in frontline healthcare settings such as the emergency department (ED). We sought to assess whether unfiltered data (containing artifacts) from a video-oculography (VOG) device have an impact on VOR gain measures in acute vestibular syndrome (AVS).
Methods: This cross-sectional study compared VOG HIT results 'unfiltered' (standard device output) versus 'filtered' (artifacts manually removed) and relative to a gold standard final diagnosis (neuroimaging plus clinical follow-up) in 23 ED patients with acute dizziness, nystagmus, gait disturbance and head motion intolerance.
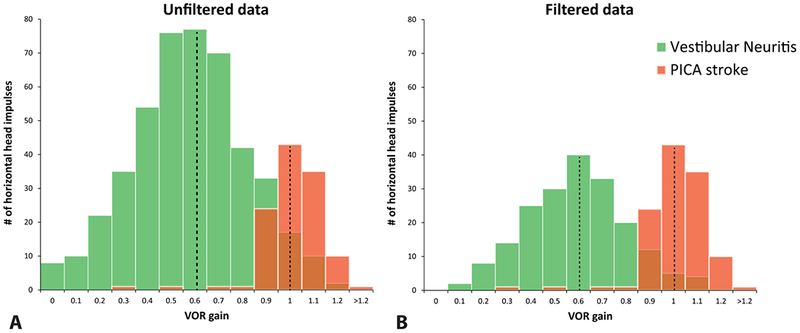
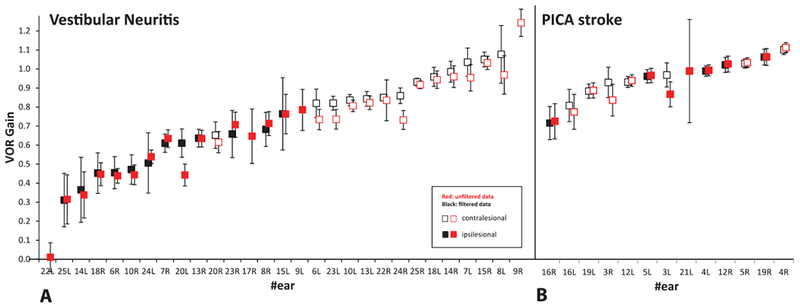
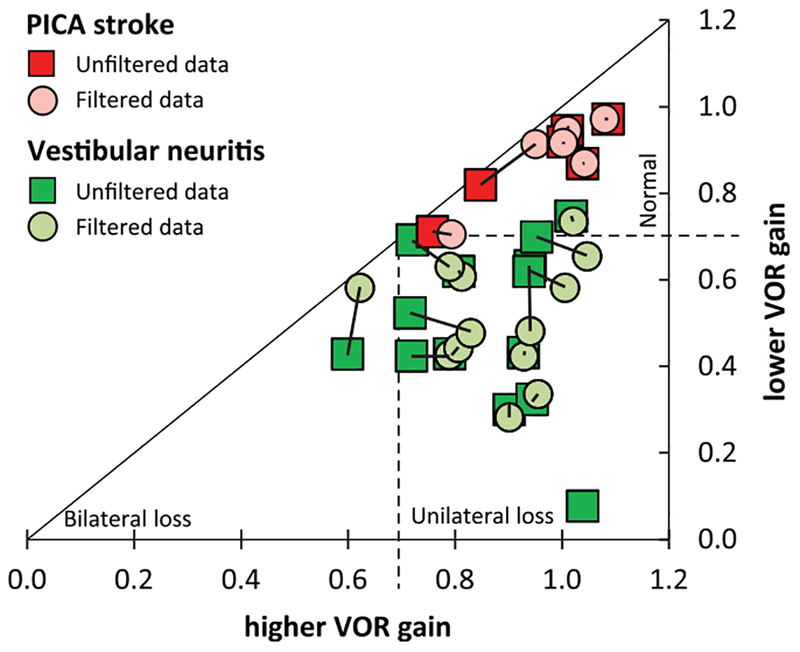
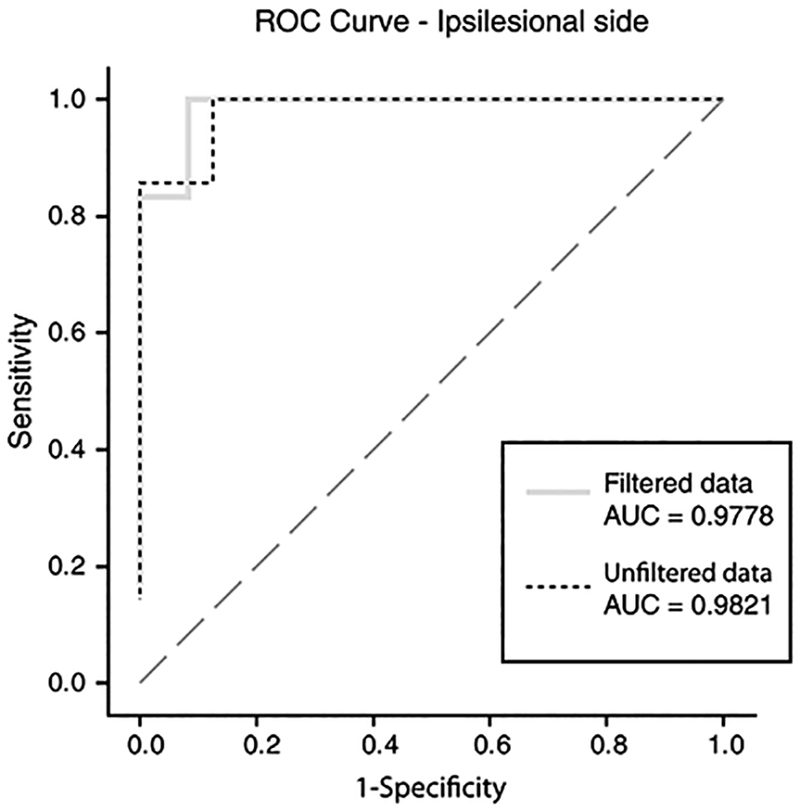
Results: Mean VOR gain assessment alone (unfiltered device data) discriminated posterior inferior cerebellar artery (PICA) strokes from vestibular neuritis with 91% accuracy in AVS. Optimal stroke discrimination cut points were bilateral VOR gain >0.7099 (unfiltered data) versus >0.7041 (filtered data). For PICA stroke sensitivity and specificity, there was no clinically-relevant difference between unfiltered and filtered data-sensitivity for PICA stroke was 100% for both data sets and specificity was almost identical (87.5% unfiltered versus 91.7% filtered). More impulses increased gain precision.
Conclusions: The bedside HIT remains the single best method for discriminating between vestibular neuritis and PICA stroke in patients presenting AVS. Quantitative VOG HIT testing in the ED is associated with frequent artifacts that reduce precision but not accuracy. At least 10-20 properly-performed HIT trials per tested ear are recommended for a precise VOR gain estimate.
Keywords: Eye movement measurements; diagnosis; stroke; vertigo; vestibular neuritis; vestibulo-ocular reflex.
Conflict of interest statement
Potential conflicts of interest
None.
Figures

References
-
- Aw ST, Fetter M, Cremer PD, Karlberg M and Halmagyi GM, Individual semicircular canal function in superior and inferior vestibular neuritis, Neurology 57 (2001), 768–774. - PubMed
-
- Beynon GJ, Jani P and Baguley DM, A clinical evaluation of head impulse testing, Clin Otolaryngol Allied Sci 23 (1998), 117–122. - PubMed
-
- Chen L, Lee W, Chambers BR and Dewey HM, Diagnostic accuracy of acute vestibular syndrome at the bedside in a stroke unit, J Neurol 258 (2011), 855–861. - PubMed
-
- Cnyrim CD, Newman-Toker D, Karch C, Brandt T and Strupp M, Bedside differentiation of vestibular neuritis from central vestibular pseudoneuritis, J Neurol Neurosurg Psychiatry 79 (2008), 458–460. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
