

Scaling-up the use of sulfadoxine-pyrimethamine for the preventive treatment of malaria in pregnancy: results and lessons on scalability, costs and programme impact from three local government areas in Sokoto State, Nigeria
- PMID: 27814763
- PMCID: PMC5097385
- DOI: 10.1186/s12936-016-1578-x
Scaling-up the use of sulfadoxine-pyrimethamine for the preventive treatment of malaria in pregnancy: results and lessons on scalability, costs and programme impact from three local government areas in Sokoto State, Nigeria
Abstract
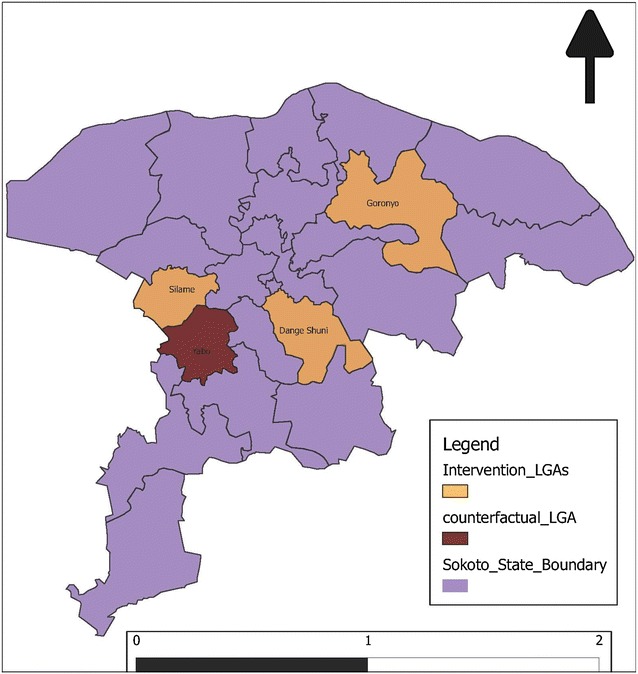
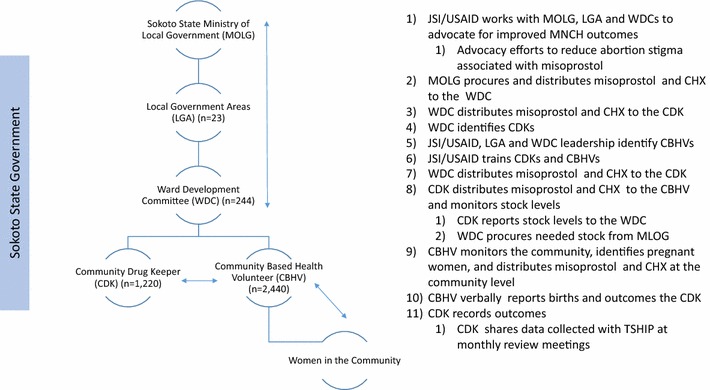
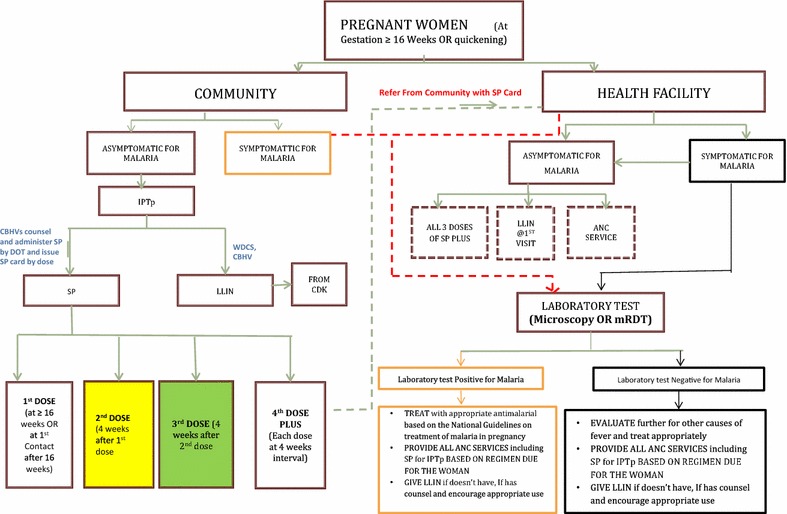
Background: Intermittent preventive treatment of malaria in pregnancy with 3+ doses of sulfadoxine-pyrimethamine (IPTp-SP) reduces maternal mortality and stillbirths in malaria endemic areas. Between December 2014 and December 2015, a project to scale up IPTp-SP to all pregnant women was implemented in three local government areas (LGA) of Sokoto State, Nigeria. The intervention included community education and mobilization, household distribution of SP, and community health information systems that reminded mothers of upcoming SP doses. Health facility IPTp-SP distribution continued in three intervention (population 661,606) and one counterfactual (population 167,971) LGAs. During the project lifespan, 31,493 pregnant women were eligible for at least one dose of IPTp-SP.
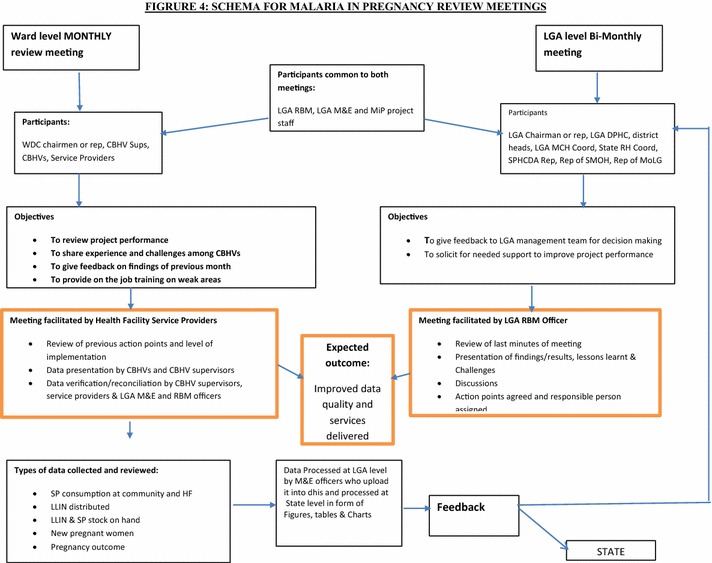
Methods: Community and facility data on IPTp-SP distribution were collected in all four LGAs. Data from a subset of 9427 pregnant women, who were followed through 42 days postpartum, were analysed to assess associations between SP dosages and newborn status. Nominal cost and expense data in 2015 Nigerian Naira were obtained from expenditure records on the distribution of SP.
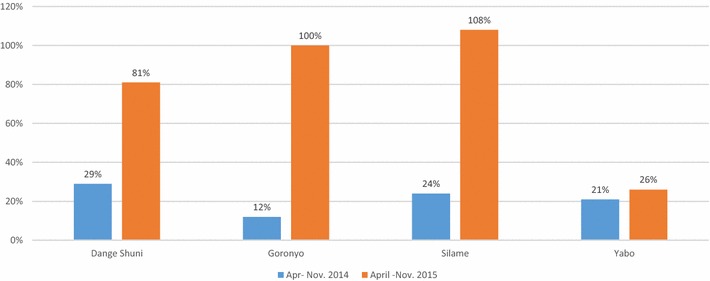
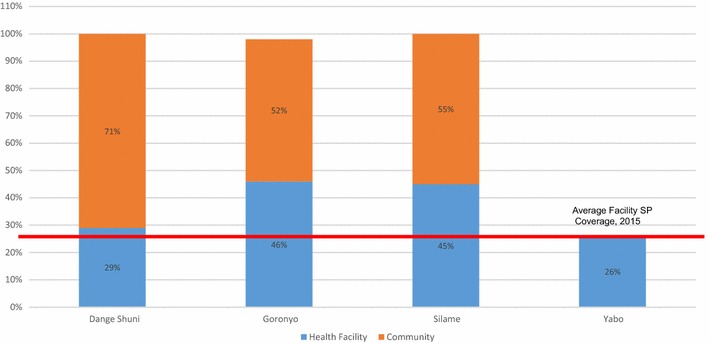
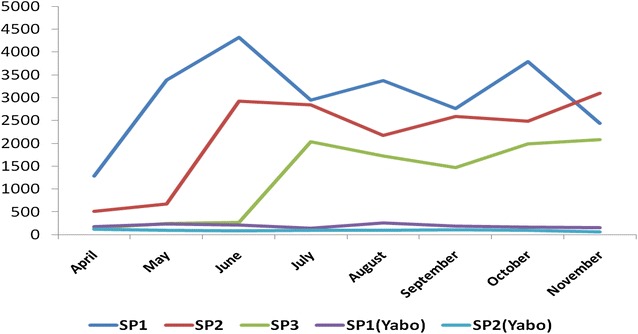
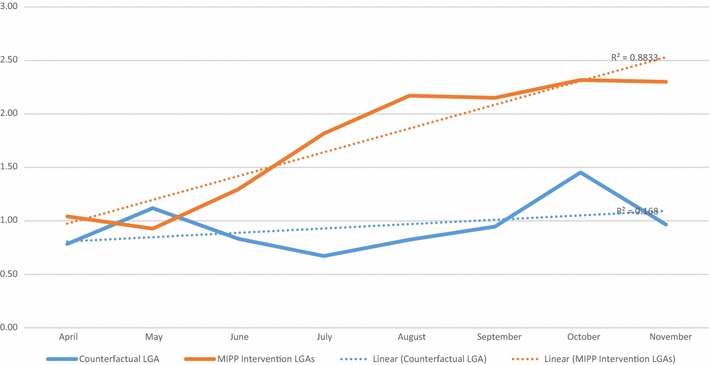
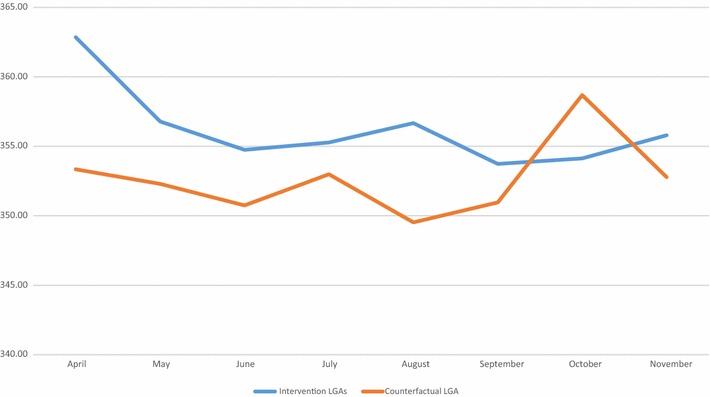
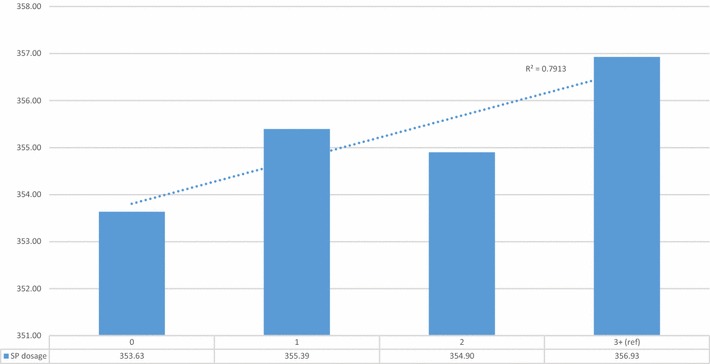
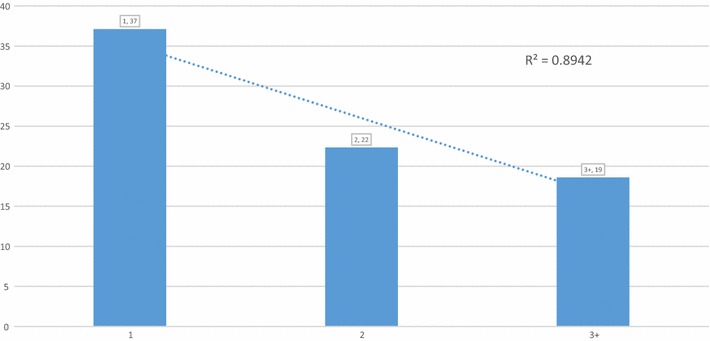
Results: Eighty-two percent (n = 25,841) of eligible women received one or more doses of IPTp-SP. The SP1 coverage was 95% in the intervention LGAs; 26% in the counterfactual. Measurable SP3+ coverage was 45% in the intervention and 0% in the counterfactual LGAs. The mean number of SP doses in the intervention LGAs was 2.1; 0.4 in the counterfactual. Increased doses of IPTp-SP were associated with linear increases in newborn head circumference and lower odds of stillbirth. Any antenatal care utilization predicted larger newborn head circumference and lower odds of stillbirth. The cost of delivering three doses of SP, inclusive of the cost of medicines, was US$0.93-$1.20.
Conclusions: It is feasible, safe, and affordable to scale up the delivery of high impact IPTp-SP interventions in low resource malaria endemic settings, where few women access facility-based maternal health services. ClinicalTrials.gov Identifier NCT02758353. Registered 29 April 2016, retrospectively registered.
Keywords: Community engagement; Community-based health workers; Human-centered design; IPTp-SP; Integrated MNH; Malaria in pregnancy; Nigeria; Primary health care; Scale up; Sokoto State.
Figures
References
-
- WHO. 10 facts on malaria. Geneva: World Health Organization; 2015. http://www.who.int/features/factfiles/malaria/en/. Accessed 21 Feb 2016.
-
- WHO. World Malaria Report 2015. Geneva: World Health Organization; 2015. http://apps.who.int/iris/bitstream/10665/200018/1/9789241565158_eng.pdf?.... Accessed 15 Feb 2016.
-
- Roll Back Malaria Partnership. Progress and impact series: country reports, country reports No. 4. Focus on Nigeria. 2012. http://www.rollbackmalaria.org/files/files/resources/report11-en.pdf. Accessed 10 Feb 2016.
-
- Nigeria population 2016. Current population of Nigeria. 2016. http://countrymeters.info/en/Nigeria. Accessed 8 Oct 2016.
-
- WHO. Malaria in pregnant women. Geneva: World Health Organization; 2016. http://www.who.int/malaria/areas/high_risk_groups/pregnancy/en/. Accessed 8 Oct 2016.
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
