

The effect of a conditional cash transfer on HIV incidence in young women in rural South Africa (HPTN 068): a phase 3, randomised controlled trial
- PMID: 27815148
- PMCID: PMC5626439
- DOI: 10.1016/S2214-109X(16)30253-4
The effect of a conditional cash transfer on HIV incidence in young women in rural South Africa (HPTN 068): a phase 3, randomised controlled trial
Erratum in
-
Correction to Lancet Glob Health 2016; 4: e978-88.Lancet Glob Health. 2017 Feb;5(2):e146. doi: 10.1016/S2214-109X(16)30361-8. Lancet Glob Health. 2017. PMID: 28104183 No abstract available.
Abstract
Background: Cash transfers have been proposed as an intervention to reduce HIV-infection risk for young women in sub-Saharan Africa. However, scarce evidence is available about their effect on reducing HIV acquisition. We aimed to assess the effect of a conditional cash transfer on HIV incidence among young women in rural South Africa.
Methods: We did a phase 3, randomised controlled trial (HPTN 068) in the rural Bushbuckridge subdistrict in Mpumalanga province, South Africa. We included girls aged 13-20 years if they were enrolled in school grades 8-11, not married or pregnant, able to read, they and their parent or guardian both had the necessary documentation necessary to open a bank account, and were residing in the study area and intending to remain until trial completion. Young women (and their parents or guardians) were randomly assigned (1:1), by use of numbered sealed envelopes containing a randomisation assignment card which were numerically ordered with block randomisation, to receive a monthly cash transfer conditional on school attendance (≥80% of school days per month) versus no cash transfer. Participants completed an Audio Computer-Assisted Self-Interview (ACASI), before test HIV counselling, HIV and herpes simplex virus (HSV)-2 testing, and post-test counselling at baseline, then at annual follow-up visits at 12, 24, and 36 months. Parents or guardians completed a Computer-Assisted Personal Interview at baseline and each follow-up visit. A stratified proportional hazards model was used in an intention-to-treat analysis of the primary outcome, HIV incidence, to compare the intervention and control groups. This study is registered at ClinicalTrials.gov (NCT01233531).
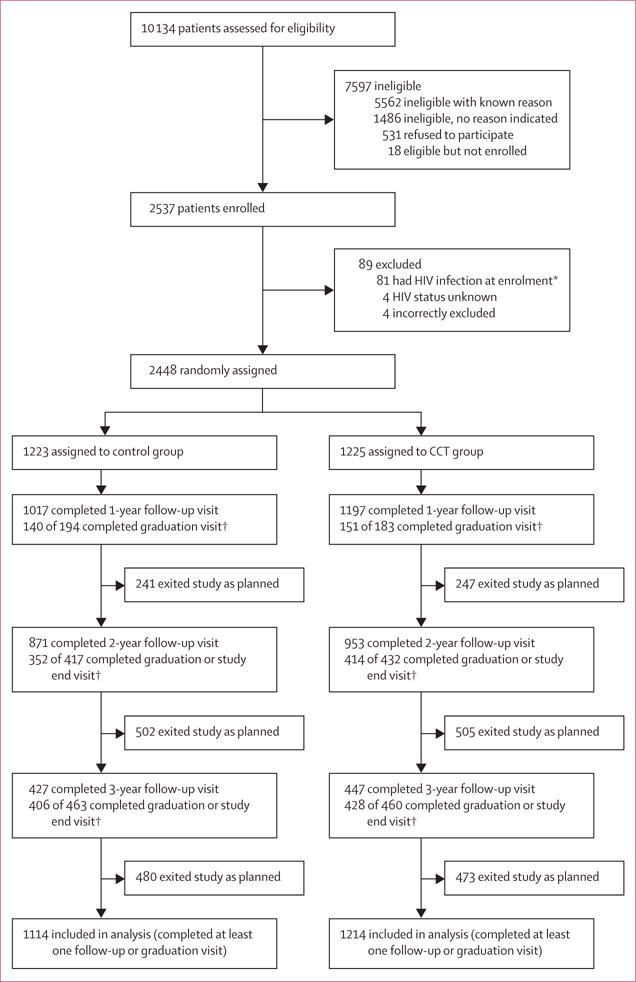
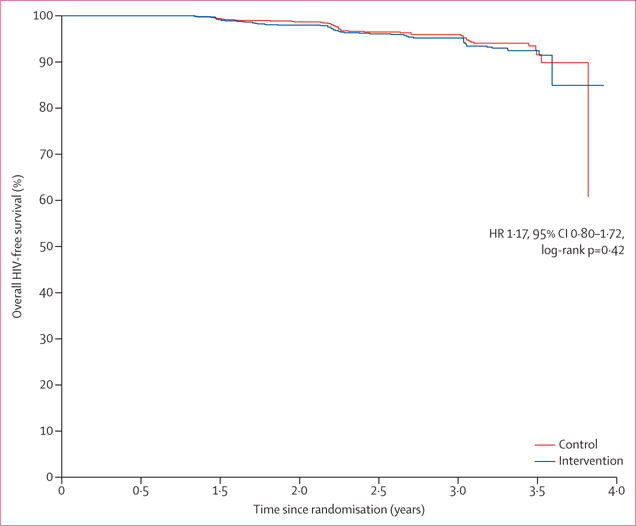
Findings: Between March 5, 2011, and Dec 17, 2012, we recruited 10 134 young women and enrolled 2537 and their parents or guardians to receive a cash transfer programme (n=1225) or not (control group; n=1223). At baseline, the median age of girls was 15 years (IQR 14-17) and 672 (27%) had reported to have ever had sex. 107 incident HIV infections were recorded during the study: 59 cases in 3048 person-years in the intervention group and 48 cases in 2830 person-years in the control group. HIV incidence was not significantly different between those who received a cash transfer (1·94% per person-years) and those who did not (1·70% per person-years; hazard ratio 1·17, 95% CI 0·80-1·72, p=0·42).
Interpretation: Cash transfers conditional on school attendance did not reduce HIV incidence in young women. School attendance significantly reduced risk of HIV acquisition, irrespective of study group. Keeping girls in school is important to reduce their HIV-infection risk.
Funding: National Institute of Allergy and Infectious Diseases, National Institute of Mental Health of the National Institutes of Health.
Copyright © 2016 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
We declare no competing interests.
Figures
Comment in
-
Cash transfers-magic bullet or fundamental ingredient?Lancet Glob Health. 2016 Dec;4(12):e883-e884. doi: 10.1016/S2214-109X(16)30295-9. Epub 2016 Nov 1. Lancet Glob Health. 2016. PMID: 27815147 No abstract available.
References
-
- Shisana O, Rehle T, Simbayi LC, et al. South African National HIV prevalence, incidence and behaviour survey 2012. Cape Town: HSRC Press; 2014.
-
- Pettifor AE, Rees HV, Kleinschmidt I, et al. Young people’s sexual health in South Africa: HIV prevalence and sexual behaviors from a nationally representative household survey. AIDS. 2005;19:1525–34. - PubMed
-
- UNAIDS. The gap report. Geneva: UNAIDS; 2014.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
