

Estimating Longitudinal Risks and Benefits From Cardiovascular Preventive Therapies Among Medicare Patients: The Million Hearts Longitudinal ASCVD Risk Assessment Tool: A Special Report From the American Heart Association and American College of Cardiology
- PMID: 27815375
- PMCID: PMC6027623
- DOI: 10.1161/CIR.0000000000000467
Estimating Longitudinal Risks and Benefits From Cardiovascular Preventive Therapies Among Medicare Patients: The Million Hearts Longitudinal ASCVD Risk Assessment Tool: A Special Report From the American Heart Association and American College of Cardiology
Erratum in
-
Correction to: Estimating Longitudinal Risks and Benefits From Cardiovascular Preventive Therapies Among Medicare Patients: The Million Hearts Longitudinal ASCVD Risk Assessment Tool: A Special Report From the American Heart Association and American College of Cardiology.Circulation. 2017 Mar 28;135(13):e824-e825. doi: 10.1161/CIR.0000000000000492. Circulation. 2017. PMID: 28348099 No abstract available.
Abstract
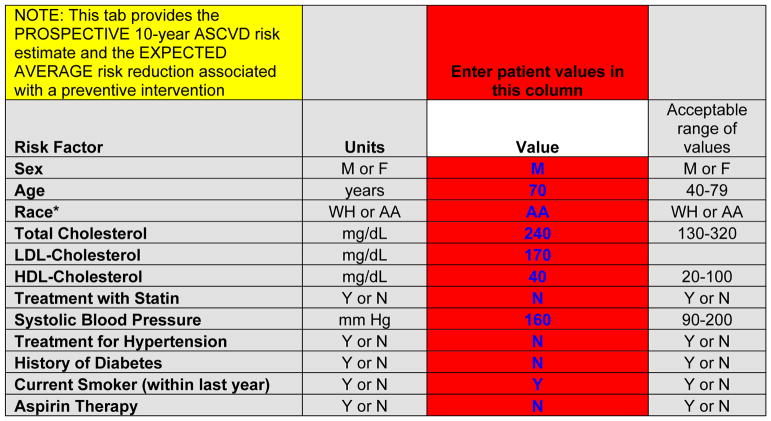
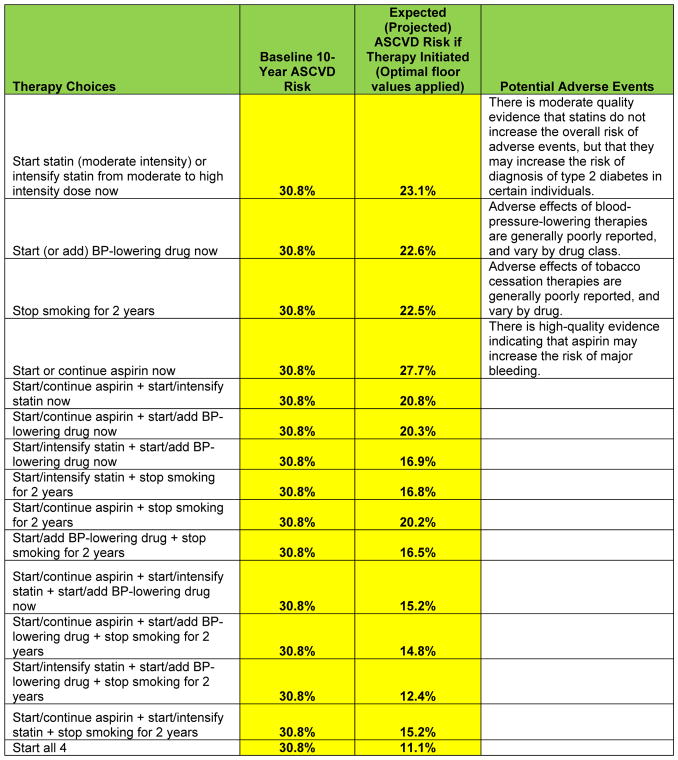
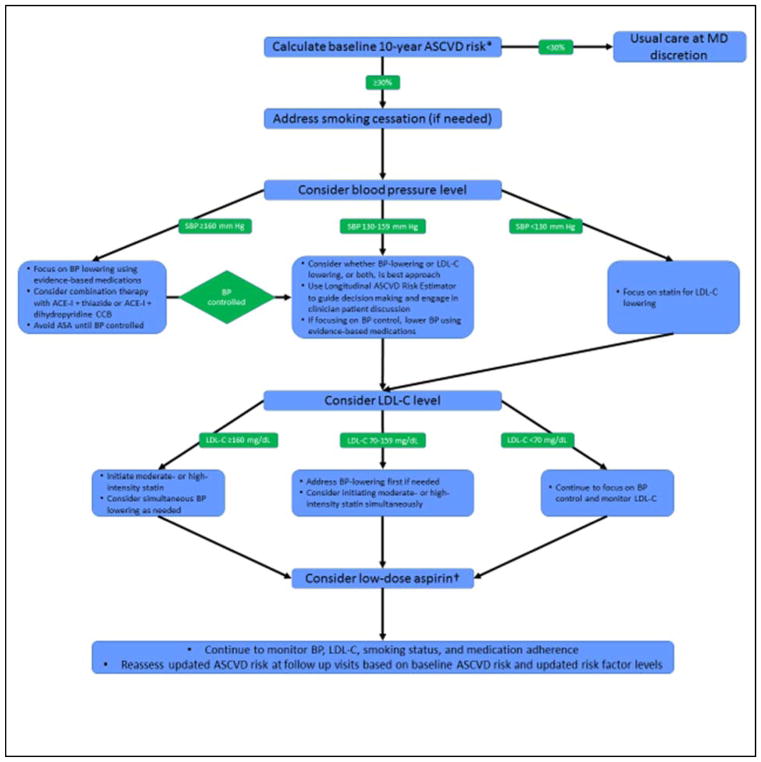
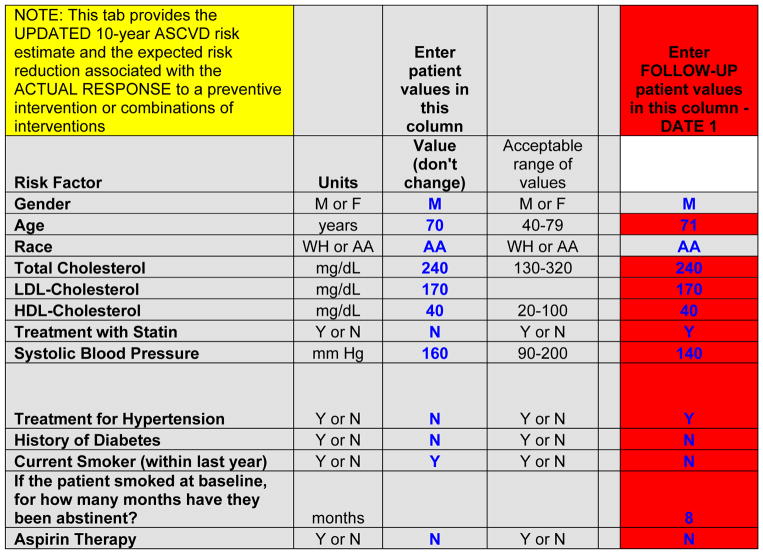
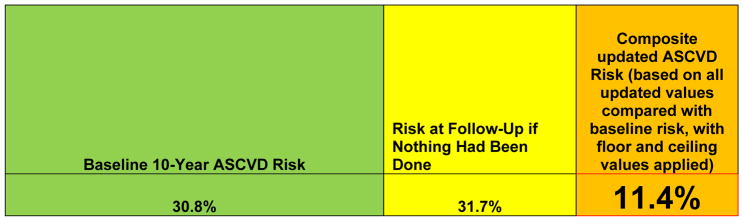
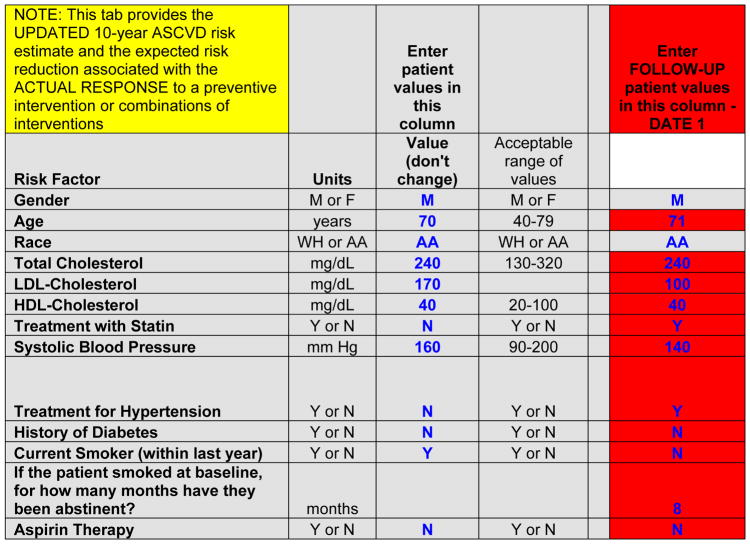
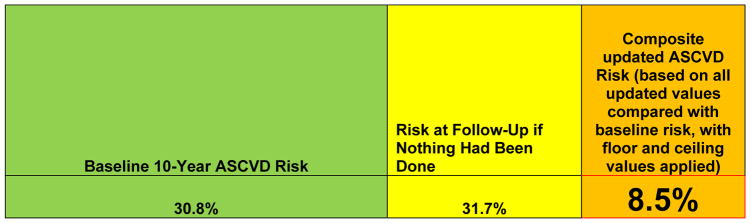
The Million Hearts Initiative has a goal of preventing 1 million heart attacks and strokes-the leading causes of mortality-through several public health and healthcare strategies by 2017. The American Heart Association and American College of Cardiology support the program. The Cardiovascular Risk Reduction Model was developed by Million Hearts and the Center for Medicare & Medicaid Services as a strategy to assess a value-based payment approach toward reduction in 10-year predicted risk of atherosclerotic cardiovascular disease (ASCVD) by implementing cardiovascular preventive strategies to manage the "ABCS" (aspirin therapy in appropriate patients, blood pressure control, cholesterol management, and smoking cessation). The purpose of this special report is to describe the development and intended use of the Million Hearts Longitudinal ASCVD Risk Assessment Tool. The Million Hearts Tool reinforces and builds on the "2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk" by allowing clinicians to estimate baseline and updated 10-year ASCVD risk estimates for primary prevention patients adhering to the appropriate ABCS over time, alone or in combination. The tool provides updated risk estimates based on evidence from high-quality systematic reviews and meta-analyses of the ABCS therapies. This novel approach to personalized estimation of benefits from risk-reducing therapies in primary prevention may help target therapies to those in whom they will provide the greatest benefit, and serves as the basis for a Center for Medicare & Medicaid Services program designed to evaluate the Million Hearts Cardiovascular Risk Reduction Model.
Keywords: AHA Scientific Statements; cardiovascular diseases; morbidity; mortality; myocardial infarction; population; prevention; stroke.
© 2016 by the American Heart Association, Inc., and the American College of Cardiology Foundation.
Figures

References
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Despres JP, Fullerton HJ, Howard VJ, Huffman MD, Isasi CR, Jimenez MC, Judd SE, Kissela BM, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Magid DJ, McGuire DK, Mohler ER, 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Rosamond W, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Woo D, Yeh RW, Turner MB on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation. 2016;133:e38–e360. [published correction appears in Circulation 2016;133:e599] - PubMed
-
- Weintraub WS, Daniels SR, Burke LE, Franklin BA, Goff DC, Jr, Hayman LL, Lloyd-Jones D, Pandey DK, Sanchez EJ, Schram AP, Whitsel LP on behalf of the American Heart Association Advocacy Coordinating Committee; Council on Cardiovascular Disease in the Young; Council on the Kidney in Cardiovascular Disease; Council on Epidemiology and Prevention; Council on Cardiovascular Nursing; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Clinical Cardiology; and Stroke Council. Value of primordial and primary prevention for cardiovascular disease: a policy statement from the American Heart Association. Circulation. 2011;124:967–990. - PubMed
-
- Frieden TR, Berwick DM. The “Million Hearts” initiative--preventing heart attacks and strokes. N Engl J Med. 2011;365:e27. - PubMed
-
- [Accessed August 1, 2016];Million Hearts website. Available at: http://millionhearts.hhs.gov/
-
- Sanghavi DM, Conway PH. Paying for prevention: a novel test of Medicare value-based payment for cardiovascular risk reduction. JAMA. 2015;314:123–124. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
