

Developing a robotic colorectal cancer surgery program: understanding institutional and individual learning curves
- PMID: 27815742
- PMCID: PMC5418100
- DOI: 10.1007/s00464-016-5292-0
Developing a robotic colorectal cancer surgery program: understanding institutional and individual learning curves
Abstract
Importance: Robotic colorectal resection continues to gain in popularity. However, limited data are available regarding how surgeons gain competency and institutions develop programs.
Objective: To determine the number of cases required for establishing a robotic colorectal cancer surgery program.
Design: Retrospective review.
Setting: Cancer center.
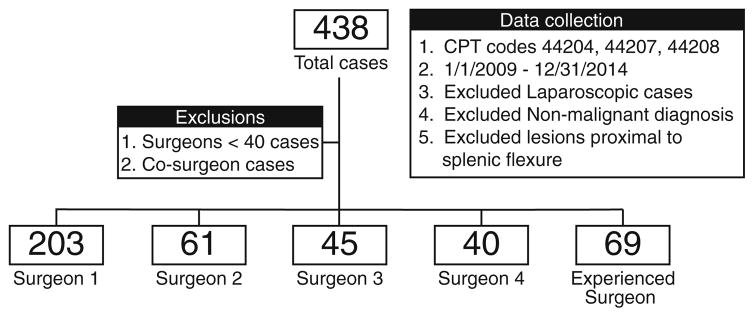
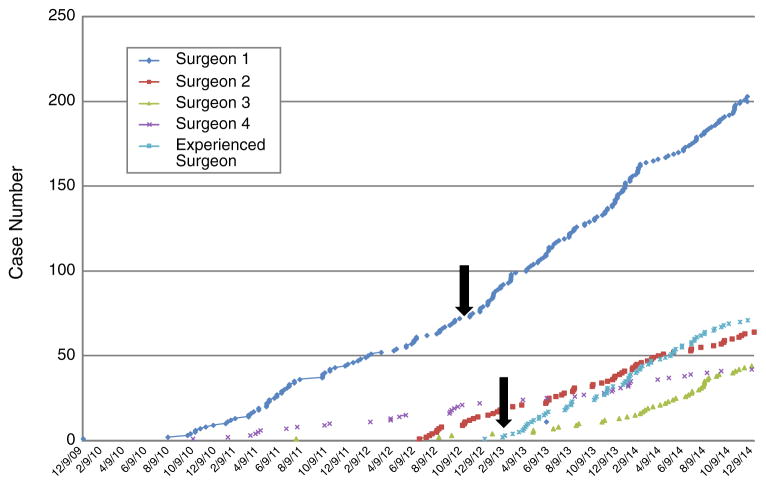
Patients: We reviewed 418 robotic-assisted resections for colorectal adenocarcinoma from January 1, 2009, to December 31, 2014, by surgeons at a single institution. The individual surgeon's and institutional learning curve were examined. The earliest adopter, Surgeon 1, had the highest volume. Surgeons 2-4 were later adopters. Surgeon 5 joined the group with robotic experience.
Interventions: A cumulative summation technique (CUSUM) was used to construct learning curves and define the number of cases required for the initial learning phase. Perioperative variables were analyzed across learning phases.
Main outcome measure: Case numbers for each stage of the learning curve.
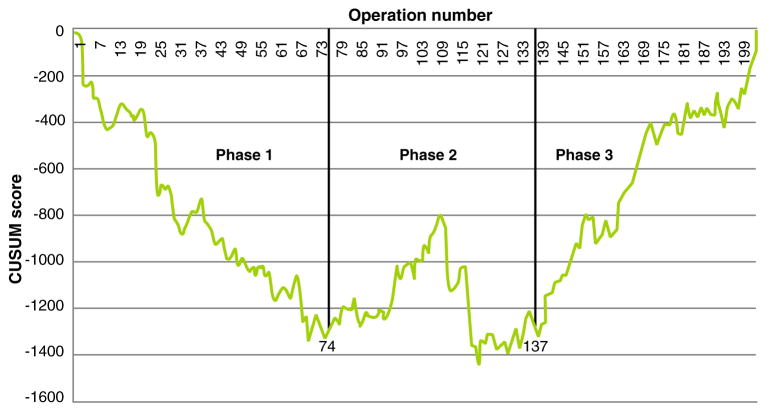
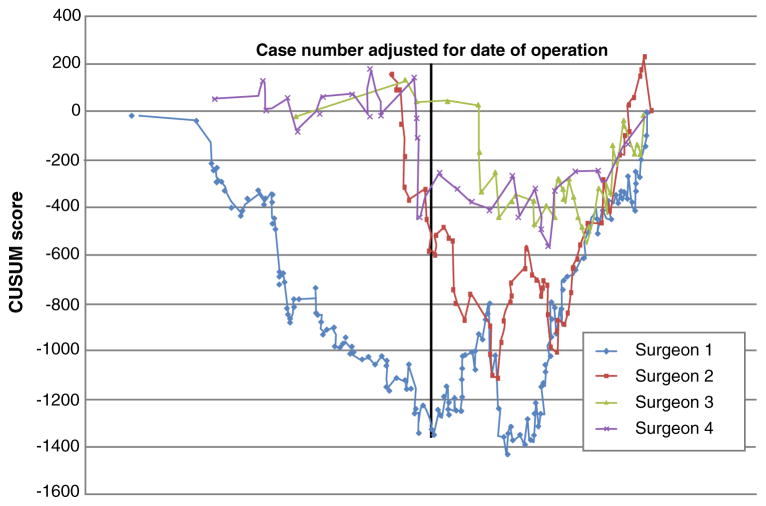
Results: The earliest adopter, Surgeon 1, performed 203 cases. CUSUM analysis of surgeons' experience defined three learning phases, the first requiring 74 cases. Later adopters required 23-30 cases for their initial learning phase. For Surgeon 1, operative time decreased from 250 to 213.6 min from phase 1-3 (P = 0.008), with no significant changes in intraoperative complication or leak rate. For Surgeons 2-4, operative time decreased from 418 to 361.9 min across the two phases (P = 0.004). Their intraoperative complication rate decreased from 7.8 to 0 % (P = 0.03); the leak rate was not significantly different (9.1 vs. 1.5 %, P = 0.07), though it may be underpowered given the small number of events.
Conclusions: Our data suggest that establishing a robotic colorectal cancer surgery program requires approximately 75 cases. Once a program is well established, the learning curve is shorter and surgeons require fewer cases (25-30) to reach proficiency. These data suggest that the institutional learning curve extends beyond a single surgeon's learning experience.
Keywords: Laparoscopy; Learning curve; Rectal cancer; Robotics.
Figures
References
-
- Weber PA, Merola S, Wasielewki A, Ballantyne GH. Telerobotic-assisted laparoscopic right and sigmoid colectomies for benign disease. Dis Colon Rectum. 2002;45(12):1689–1694. - PubMed
-
- Pigazzi A, Elllenhorn JD, Ballantyne GH, Paz IB. Robotic-assisted laparoscopic low anterior resection with total mesorectal excision for rectal cancer. Surg Endosc. 2006;20(10):1521–1525. - PubMed
-
- Wexner SD, Bergamaschi R, Lacy A, et al. The current status of robotic pelvic surgery: results of a multinational interdisciplinary consensus conference. Surg Endosc. 2009;23(2):438–443. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
