

Predictive value of the Status Epilepticus Severity Score (STESS) and its components for long-term survival
- PMID: 27816063
- PMCID: PMC5097843
- DOI: 10.1186/s12883-016-0730-0
Predictive value of the Status Epilepticus Severity Score (STESS) and its components for long-term survival
Abstract
Background: The "Status Epilepticus Severity Score" (STESS) is the most important clinical score to predict in-hospital mortality of patients with status epilepticus (SE), but its prognostic relevance for long-term survival is unknown. This study therefore examined if STESS and its components retain their prognostic relevance beyond acute treatment.
Methods: One hundred twenty-five non-anoxic patients with SE were retrospectively identified in two hospitals between 2008 and 2014 (39.2 % refractory SE). Patients' treatment, demographic data, date of death, aetiology of SE, and the components of the STESS (age, history of seizures, level of consciousness and worst seizure type) were determined based on the patients' records.
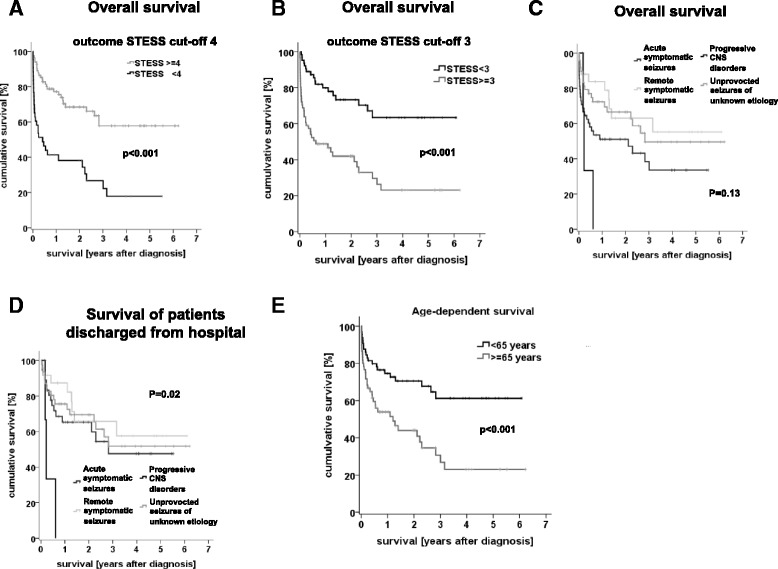
Results: In 94.4 % of patients, SE was treated successfully; in-hospital mortality rate was 12 %. The overall mortality was 42 % after median follow-up of 28.1 months. The survival plateaued after about 3 years, all patients with progressive brain diseases (n = 4) died within one year. In-hospital mortality correlated highly significantly with STESS, the optimal cut-off was 4. With respect to long-term outcome, STESS correlated significantly with overall mortality though with lower odds ratios. When looking only at patients that survived the acute phase of treatment, only the STESS components "level of consciousness" (at admission), "coma" as worst seizure type, and "age" reached a statistical significant association with mortality. In these patients, STESS with a cut-off of 4 was not significantly associated with survival/mortality. Aetiology of SE was insufficient to explain the weak association and the high mortality after discharge alone.
Conclusion: STESS at onset of SE reliably assessed in-hospital mortality, and was indicative for overall survival. However, STESS did not allow correct estimation of mortality after discharge. The high mortality after discharge and high overall mortality of patients diagnosed with SE was not explained by progressive brain disorders alone. Further research is needed to understand the causes for high overall mortality after SE and putative prognostic factors.
Keywords: Epilepsy; Long-term; Mortality; STESS; Short-term.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
