

Enhanced Recovery after Bariatric Surgery: Systematic Review and Meta-Analysis
- PMID: 27817086
- PMCID: PMC5187372
- DOI: 10.1007/s11695-016-2438-z
Enhanced Recovery after Bariatric Surgery: Systematic Review and Meta-Analysis
Abstract
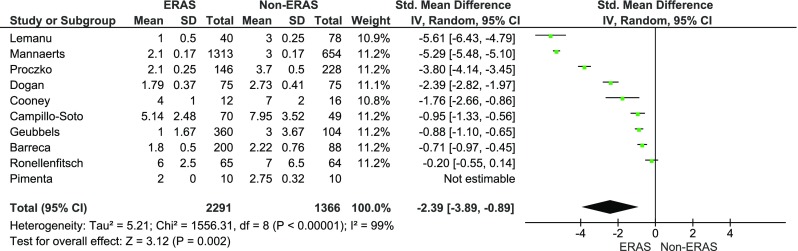
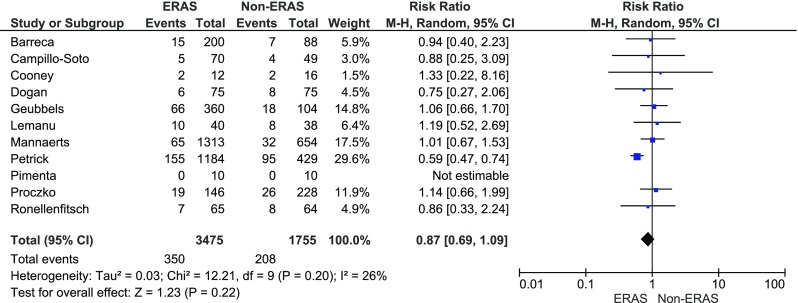
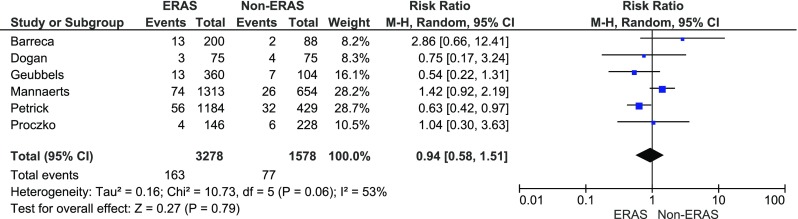
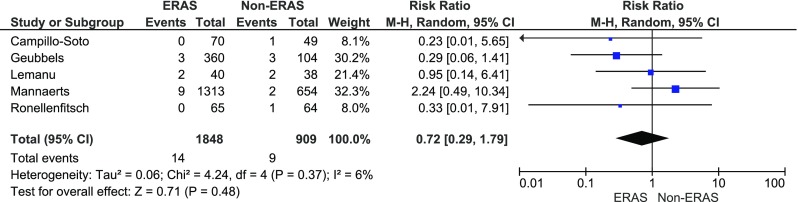
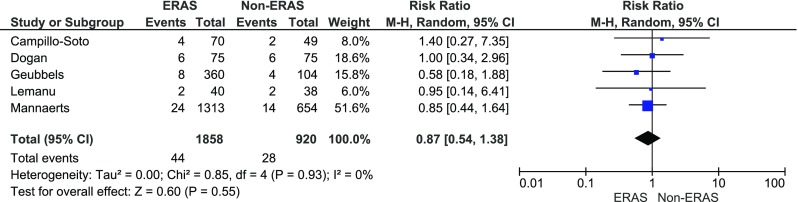
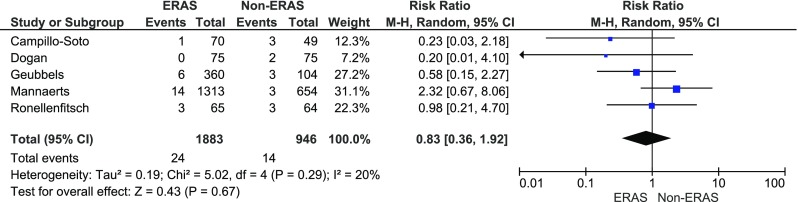
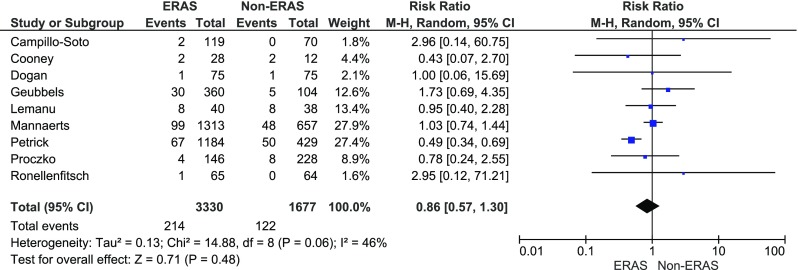
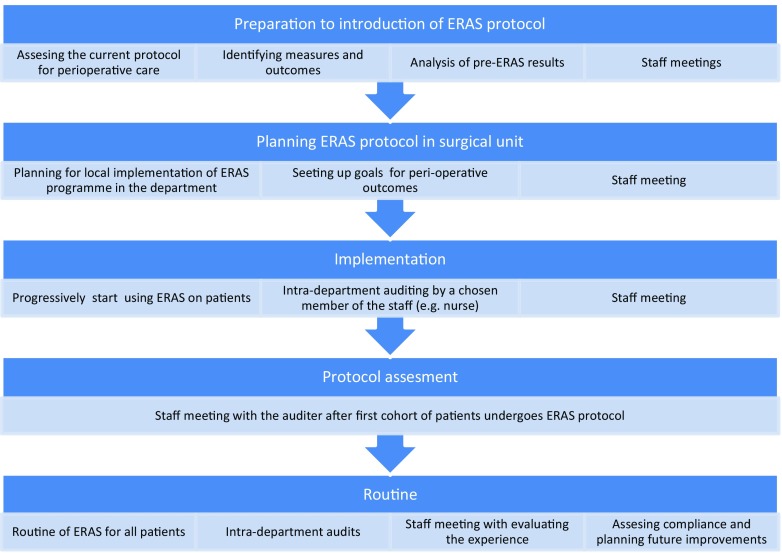
Enhanced recovery after surgery (ERAS) protocol is well established in many surgical disciplines and leads to a decrease in the length of hospital stay and morbidity. Multimodal protocols have also been introduced to bariatric surgery. This review aims to evaluate the current literature on ERAS in obesity surgery and to conduct a meta-analysis of primary and secondary outcomes. MEDLINE, Embase, Scopus and Cochrane Library were searched for eligible studies. Key journals were hand-searched. We analysed data up to May 2016. Eligible studies had to contain four described ERAS protocol elements. The primary outcome was the length of hospital stay; the secondary outcomes included overall morbidity, specific complications, mortality, readmissions and costs. Random effect meta-analyses were undertaken. The initial search yielded 1151 articles. Thorough evaluation resulted in 11 papers, which were analysed. The meta-analysis of the length of stay presented a significant reduction standard mean difference (Std. MD) = -2.39 (-3.89, -0.89), p = 0.002. The analysis of overall morbidity, specific complications and Clavien-Dindo classification showed no significant variations among the study groups. ERAS protocol in bariatric surgery leads to the reduction of the length of hospital stay while maintaining no or low influence on morbidity.
Keywords: Bariatric surgery; ERAS; Gastric bypass; Sleeve gastrectomy.
Conflict of interest statement
The authors declare that they have no conflict of interest. Ethical Approval For this type of study, formal consent is not required. Informed Consent Does not apply.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
