

Dark blood late enhancement imaging
- PMID: 27817748
- PMCID: PMC5098284
- DOI: 10.1186/s12968-016-0297-3
Dark blood late enhancement imaging
Abstract
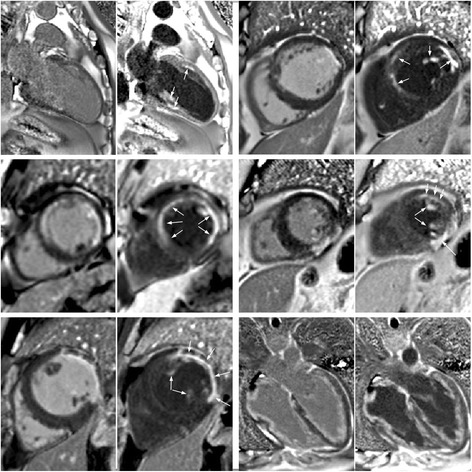
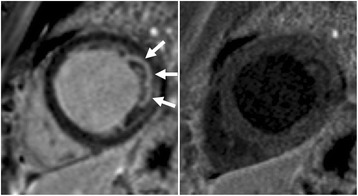
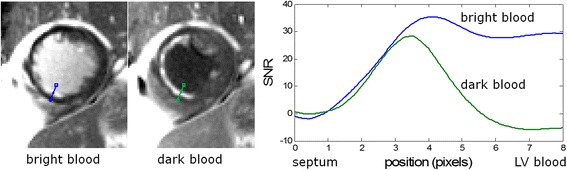
Background: Bright blood late gadolinium enhancement (LGE) imaging typically achieves excellent contrast between infarcted and normal myocardium. However, the contrast between the myocardial infarction (MI) and the blood pool is frequently suboptimal. A large fraction of infarctions caused by coronary artery disease are sub-endocardial and thus adjacent to the blood pool. It is not infrequent that sub-endocardial MIs are difficult to detect or clearly delineate.
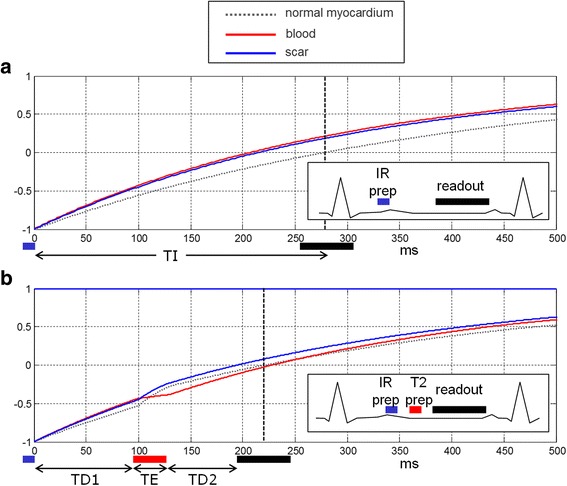
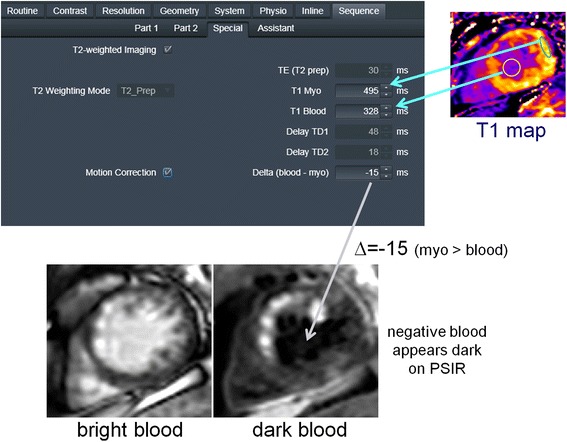
Methods: In this present work, an inversion recovery (IR) T2 preparation was combined with single shot steady state free precession imaging and respiratory motion corrected averaging to achieve dark blood LGE images with good signal to noise ratio while maintaining the desired spatial and temporal resolution. In this manner, imaging was conducted free-breathing, which has benefits for image quality, patient comfort, and clinical workflow in both adults and children. Furthermore, by using a phase sensitive inversion recovery reconstruction the blood signal may be made darker than the myocardium (i.e., negative signal values) thereby providing contrast between the blood and both the MI and remote myocardium. In the proposed approach, a single T1-map scout was used to measure the myocardial and blood T1 using a MOdified Look-Locker Inversion recovery (MOLLI) protocol and all protocol parameters were automatically calculated from these values within the sequence thereby simplifying the user interface.
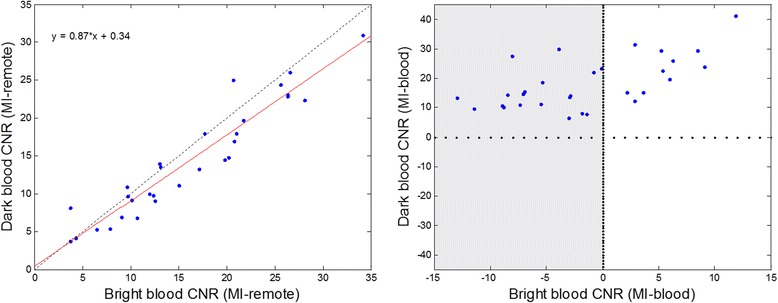
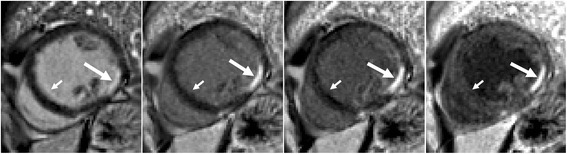
Results: The contrast to noise ratio (CNR) between MI and remote myocardium was measured in n = 30 subjects with subendocardial MI using both bright blood and dark blood protocols. The CNR for the dark blood protocol had a 13 % loss compared to the bright blood protocol. The CNR between the MI and blood pool was positive for all dark blood cases, and was negative in 63 % of the bright blood cases. The conspicuity of subendocardial fibrosis and MI was greatly improved by dark blood (DB) PSIR as well as the delineation of the subendocardial border.
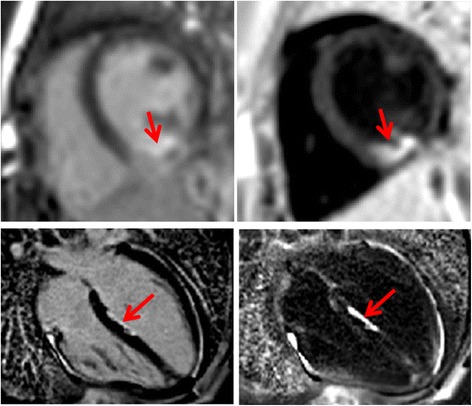
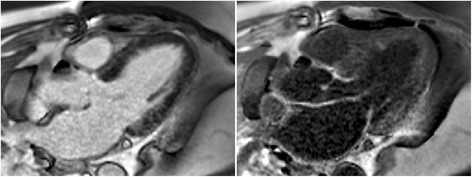
Conclusions: Free-breathing, dark blood PSIR LGE imaging was demonstrated to improve the visualization of subendocardial MI and fibrosis in cases with low contrast with adjacent blood pool. The proposed method also improves visualization of thin walled fibrous structures such as atrial walls and valves, as well as papillary muscles.
Keywords: Ablation; Dark blood; Gadolinium; LGE; Late enhancement; MOCO; Myocardial infarction; PSIR; Scar.
Figures

References
-
- Bohl S, Wassmuth R, Abdel-Aty H, Rudolph A, Messroghli D, Dietz R, et al. Delayed enhancement cardiac magnetic resonance imaging reveals typical patterns of myocardial injury in patients with various forms of non-ischemic heart disease. Int J Cardiovasc Imaging. 2008;24:597–607. doi: 10.1007/s10554-008-9300-x. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
