

Polyomavirus Reactivation and Immune Responses to Kidney-Specific Self-Antigens in Transplantation
- PMID: 27821629
- PMCID: PMC5373442
- DOI: 10.1681/ASN.2016030285
Polyomavirus Reactivation and Immune Responses to Kidney-Specific Self-Antigens in Transplantation
Abstract
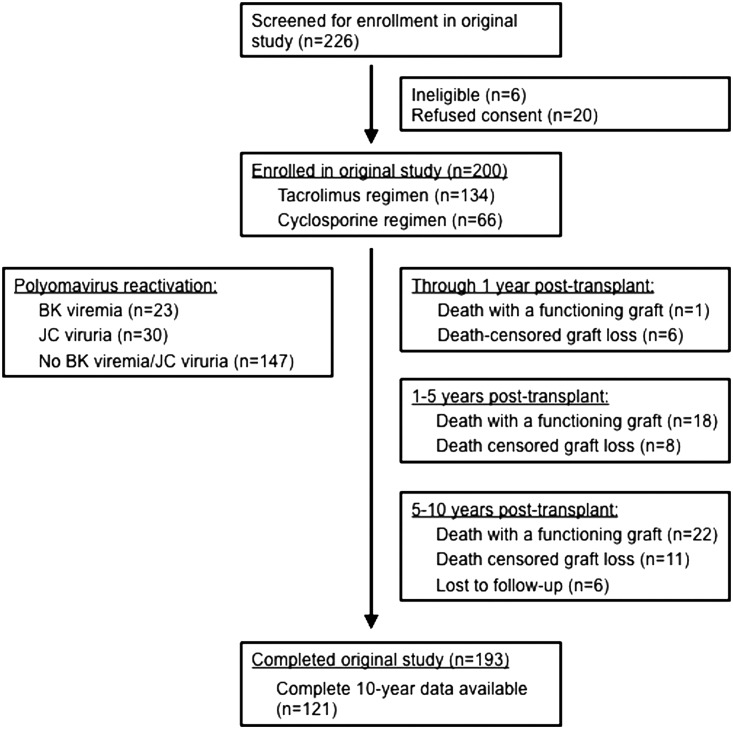
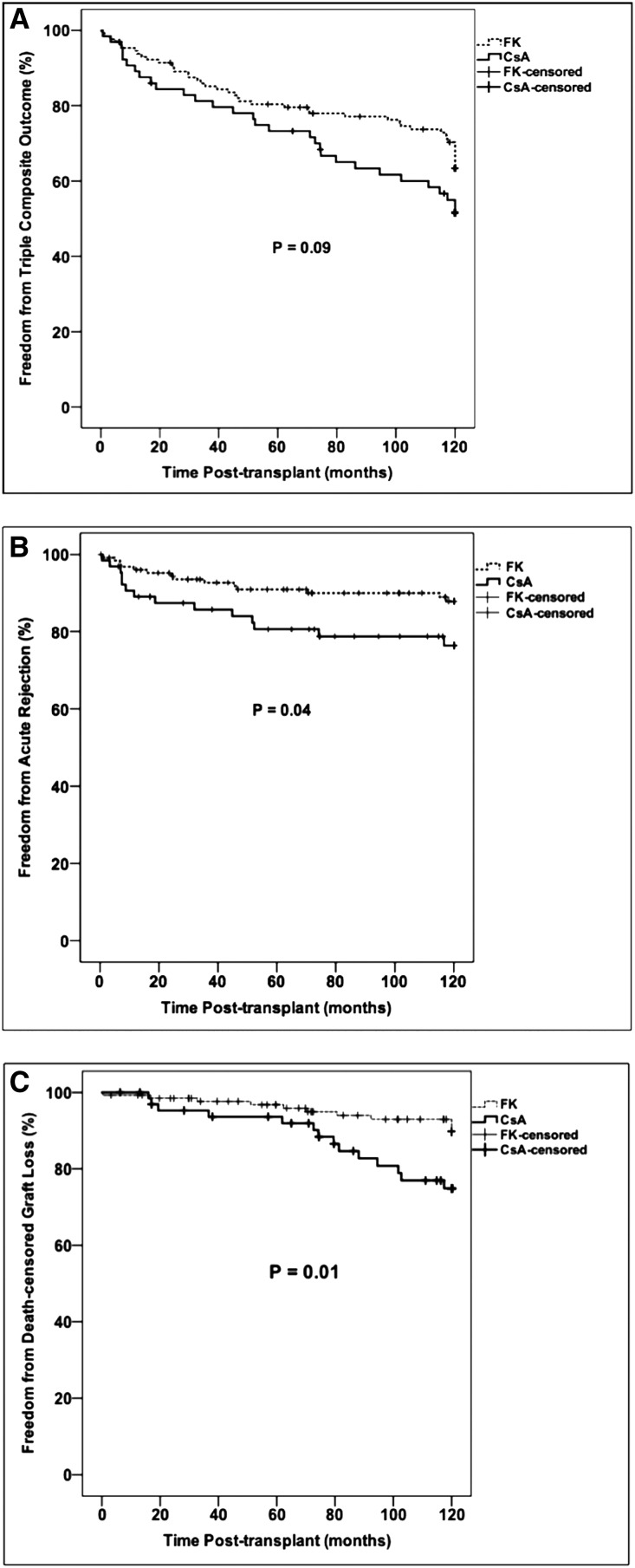
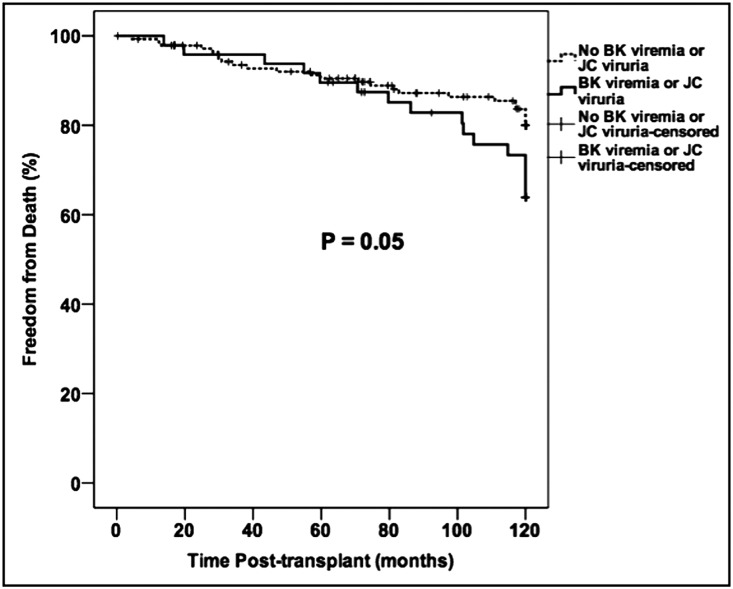
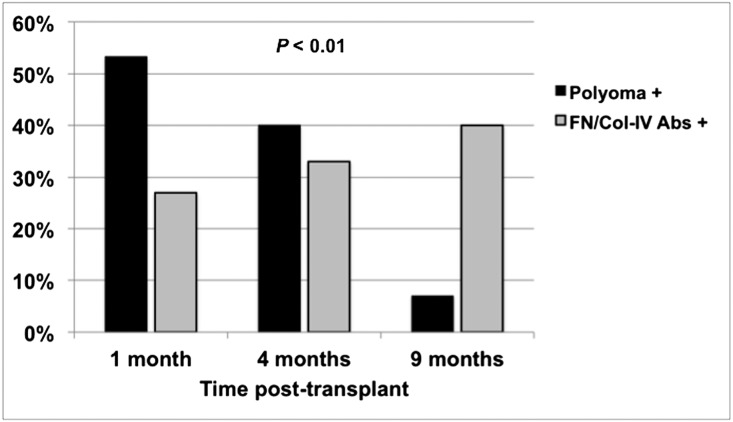
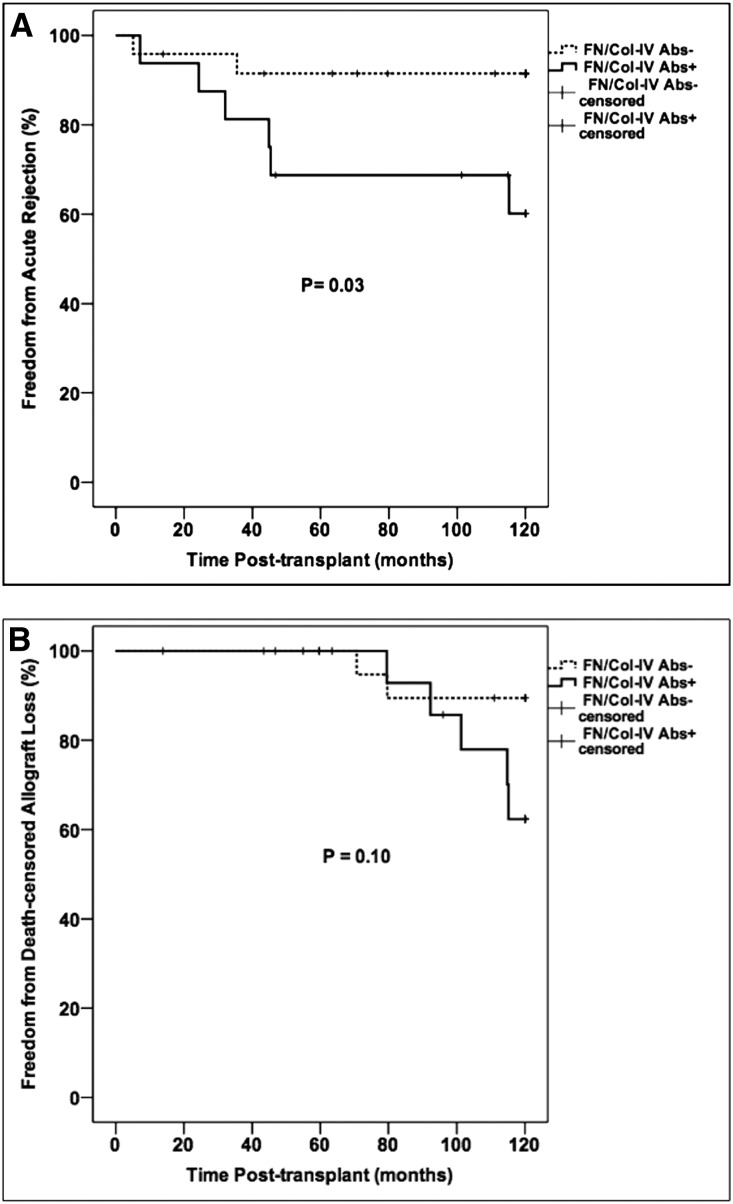
Humoral immune responses against donor antigens are important determinants of long-term transplant outcomes. Reactivation of the polyomavirus BK has been associated with de novo antibodies against mismatched donor HLA antigens in kidney transplantation. The effect of polyomavirus reactivation (BK viremia or JC viruria) on antibodies to kidney-specific self-antigens is unknown. We previously reported excellent 5-year outcomes after minimization of immunosuppression for BK viremia and after no intervention for JC viruria. Here, we report the 10-year results of this trial (n=193) along with a nested case-control study (n=40) to explore associations between polyomavirus reactivation and immune responses to the self-antigens fibronectin (FN) and collagen type-IV (Col-IV). Consistent with 5-year findings, subjects taking tacrolimus, compared with those taking cyclosporin, had less acute rejection (11% versus 22%, P=0.05) and graft loss (9% versus 22%, P=0.01) along with better transplant function (eGFR 65±19 versus 50±24 ml/min per 1.73 m2, P<0.001) at 10 years. Subjects undergoing immunosuppression reduction for BK viremia had 10-year outcomes similar to those without viremia. In the case-control study, antibodies to FN/Col-IV were more prevalent during year 1 in subjects with polyomavirus reactivation than in those without reactivation (48% versus 11%, P=0.04). Subjects with antibodies to FN/Col-IV had more acute rejection than did those without these antibodies (38% versus 8%, P=0.02). These data demonstrate the long-term safety and effectiveness of minimizing immunosuppression to treat BK viremia. Furthermore, these results indicate that polyomavirus reactivation associates with immune responses to kidney-specific self-antigens that may increase the risk for acute rejection through unclear mechanisms.
Keywords: immunosuppression; kidney transplantation; transplant outcomes; virology.
Copyright © 2017 by the American Society of Nephrology.
Figures
References
-
- Sellarés J, de Freitas DG, Mengel M, Reeve J, Einecke G, Sis B, Hidalgo LG, Famulski K, Matas A, Halloran PF: Understanding the causes of kidney transplant failure: The dominant role of antibody-mediated rejection and nonadherence. Am J Transplant 12: 388–399, 2012 - PubMed
-
- Gaston RS, Cecka JM, Kasiske BL, Fieberg AM, Leduc R, Cosio FC, Gourishankar S, Grande J, Halloran P, Hunsicker L, Mannon R, Rush D, Matas AJ: Evidence for antibody-mediated injury as a major determinant of late kidney allograft failure. Transplantation 90: 68–74, 2010 - PubMed
-
- Mannon RB, Matas AJ, Grande J, Leduc R, Connett J, Kasiske B, Cecka JM, Gaston RS, Cosio F, Gourishankar S, Halloran PF, Hunsicker L, Rush D; DeKAF Investigators : Inflammation in areas of tubular atrophy in kidney allograft biopsies: A potent predictor of allograft failure. Am J Transplant 10: 2066–2073, 2010 - PMC - PubMed
-
- Matas AJ, Leduc R, Rush D, Cecka JM, Connett J, Fieberg A, Halloran P, Hunsicker L, Cosio F, Grande J, Mannon R, Gourishankar S, Gaston R, Kasiske B: Histopathologic clusters differentiate subgroups within the nonspecific diagnoses of CAN or CR: Preliminary data from the DeKAF study. Am J Transplant 10: 315–323, 2010 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
