

PreSERVE-AMI: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial of Intracoronary Administration of Autologous CD34+ Cells in Patients With Left Ventricular Dysfunction Post STEMI
- PMID: 27821724
- PMCID: PMC5903285
- DOI: 10.1161/CIRCRESAHA.115.308165
PreSERVE-AMI: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial of Intracoronary Administration of Autologous CD34+ Cells in Patients With Left Ventricular Dysfunction Post STEMI
Abstract
Rationale: Despite direct immediate intervention and therapy, ST-segment-elevation myocardial infarction (STEMI) victims remain at risk for infarct expansion, heart failure, reinfarction, repeat revascularization, and death.
Objective: To evaluate the safety and bioactivity of autologous CD34+ cell (CLBS10) intracoronary infusion in patients with left ventricular dysfunction post STEMI.
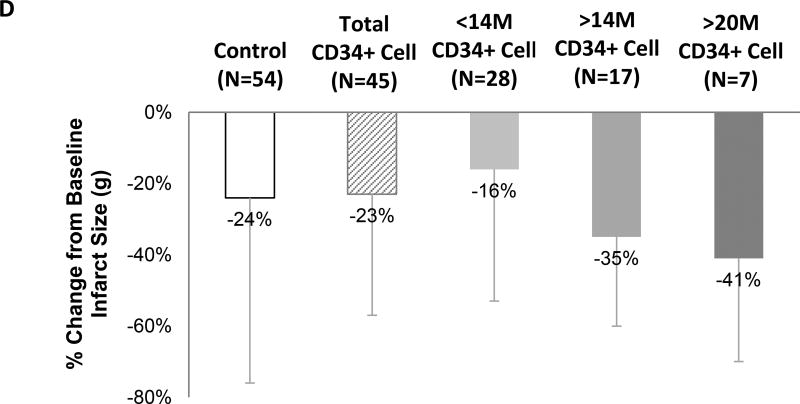
Methods and results: Patients who underwent successful stenting for STEMI and had left ventricular dysfunction (ejection fraction≤48%) ≥4 days poststent were eligible for enrollment. Subjects (N=161) underwent mini bone marrow harvest and were randomized 1:1 to receive (1) autologous CD34+ cells (minimum 10 mol/L±20% cells; N=78) or (2) diluent alone (N=83), via intracoronary infusion. The primary safety end point was adverse events, serious adverse events, and major adverse cardiac event. The primary efficacy end point was change in resting myocardial perfusion over 6 months. No differences in myocardial perfusion or adverse events were observed between the control and treatment groups, although increased perfusion was observed within each group from baseline to 6 months (P<0.001). In secondary analyses, when adjusted for time of ischemia, a consistently favorable cell dose-dependent effect was observed in the change in left ventricular ejection fraction and infarct size, and the duration of time subjects was alive and out of hospital (P=0.05). At 1 year, 3.6% (N=3) and 0% deaths were observed in the control and treatment group, respectively.
Conclusions: This PreSERVE-AMI (Phase 2, randomized, double-blind, placebo-controlled trial) represents the largest study of cell-based therapy for STEMI completed in the United States and provides evidence supporting safety and potential efficacy in patients with left ventricular dysfunction post STEMI who are at risk for death and major morbidity.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT01495364.
Keywords: cell transplantation; clinical trial; endothelial progenitor cells; heart failure; myocardial infarction.
© 2016 American Heart Association, Inc.
Figures






Comment in
-
What Is the Future of Cell-Based Therapy for Acute Myocardial Infarction.Circ Res. 2017 Jan 20;120(2):252-255. doi: 10.1161/CIRCRESAHA.116.310340. Circ Res. 2017. PMID: 28104761 Free PMC article. No abstract available.
References
-
- Solomon SD, Anavekar N, Skali H, McMurray JJ, Swedberg K, Yusuf S, Granger CB, Michelson EL, Wang D, Pocock S. Influence of ejection fraction on cardiovascular outcomes in a broad spectrum of heart failure patients. Circulation. 2005;112:3738–3744. - PubMed
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, Despres JP, Fullerton HJ, Howard VJ, Huffman MD, Judd SE, Kissela BM, Lackland DT, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Matchar DB, McGuire DK, Mohler ER, 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Willey JZ, Woo D, Yeh RW, Turner MB American Heart Association Statistics, C Stroke Statistics S. Heart disease and stroke statistics--2015 update: A report from the american heart association. Circulation. 2015;131:e29–322. - PubMed
-
- Pfeffer MA, Braunwald E. Ventricular remodeling after myocardial infarction. Experimental observations and clinical implications. Circulation. 1990;81:1161–1172. - PubMed
-
- Pfeffer MA. Left ventricular remodeling after acute myocardial infarction. Annu Rev Med. 1995;46:455–466. - PubMed
-
- Hirai T, Fujita M, Nakajima H, Asanoi H, Yamanishi K, Ohno A, Sasayama S. Importance of collateral circulation for prevention of left ventricular aneurysm formation in acute myocardial infarction. Circulation. 1989;79:791–796. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
