

PD-1 inhibition and treatment of advanced melanoma-role of pembrolizumab
- PMID: 27822406
- PMCID: PMC5088280
PD-1 inhibition and treatment of advanced melanoma-role of pembrolizumab
Abstract
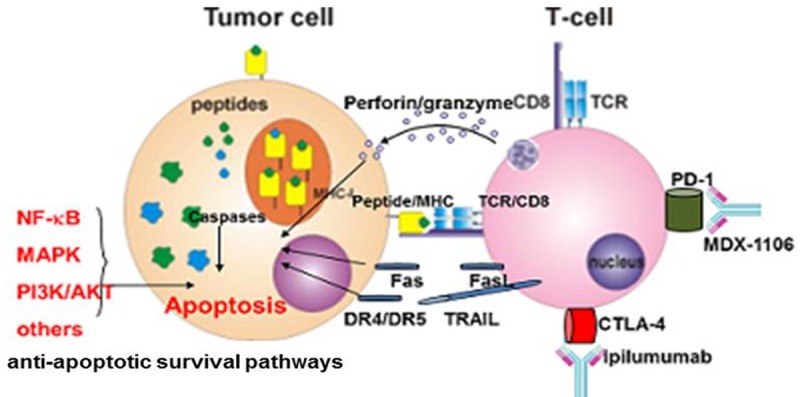
Remarkable clinical responses have been seen in patients with metastatic melanoma with targeted therapy (BRAFi vemurafenib, MEKi) and with modern immune cell-based approaches such as TCR engineered adoptive cell transfer (ACT) and earlier experiences with high-dose IL-2. The proximal mediators of these immune therapies are tumor-reactive CTL. Various mechanisms of resistance to immune-mediated apoptotic signals have been described, including phenotypic changes, effector cell exhaustion, functional tolerance, deficiencies in Ag processing and presentation, and mutation or down-regulation of antigenic epitopes. The immune system and drugs eradicate tumors via apoptosis. Therefore, tumors' resistance to apoptosis may be a determining factor that limits the efficacy of immunotherapies. It is predicted that these therapies have limited efficacy in patients whose melanomas have developed resistance to targeted therapy such as vemurafenib. Upregulation of the immune checkpoint molecule CTLA-4 on activated T cells and its interaction with CD80/86 blocks T cell activation. The fully humanized mAb ipilimumab blocks this interaction, resulting in sustained T cell stimulation. Likewise, the programmed death receptor 1 (PD-1) is another member of the B7:CD28 family of costimulatory molecules that regulates T cell activation, whose ligand (PD-L1) is expressed on melanomas. The human anti-PD-1 mAb, Pembrolizumab, overcomes tolerance, has a favorable pharmacokinetics profile with minimal undesired toxic side effects and has shown remarkable improvement in melanoma therapy. This review focuses on recent advances in the development of various anti-PD-1 checkpoint blockade antibodies and will summarize recent clinical data using immune checkpoint blocking antibodies.
Keywords: CTLA-4; MED14736; PD-1; PD-L1; Pembrolizumab; TCR; apoptosis; immunotherapy; ipilimumab; melanoma; nivolumab; tremelimumab.
Figures


References
-
- Rosenberg SA, Yang JC, Topalian SL, Schwartzentruber DJ, Weber JS, Parkinson DR, Seipp CA, Einhorn JH, White DE. Treatment of 283 consecutive patients with metastatic melanoma or renal cell cancer using high-dose bolus interleukin 2. JAMA. 1994;271:907–913. - PubMed
-
- Legha SS, Gianan MA, Plager C, Eton OE, Papadopoulos NE. Evaluation of Interleukin-2 administered by continuous infusion in patients with metastatic melanoma. Cancer. 1996;77:89–96. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials