

Optimal Volume of Administration of Intranasal Midazolam in Children: A Randomized Clinical Trial
- PMID: 27823876
- PMCID: PMC5406242
- DOI: 10.1016/j.annemergmed.2016.08.450
Optimal Volume of Administration of Intranasal Midazolam in Children: A Randomized Clinical Trial
Abstract
Study objective: The optimal intranasal volume of administration for achieving timely and effective sedation in children is unclear. We aimed to compare clinical outcomes relevant to procedural sedation associated with using escalating volumes of administration to administer intranasal midazolam.
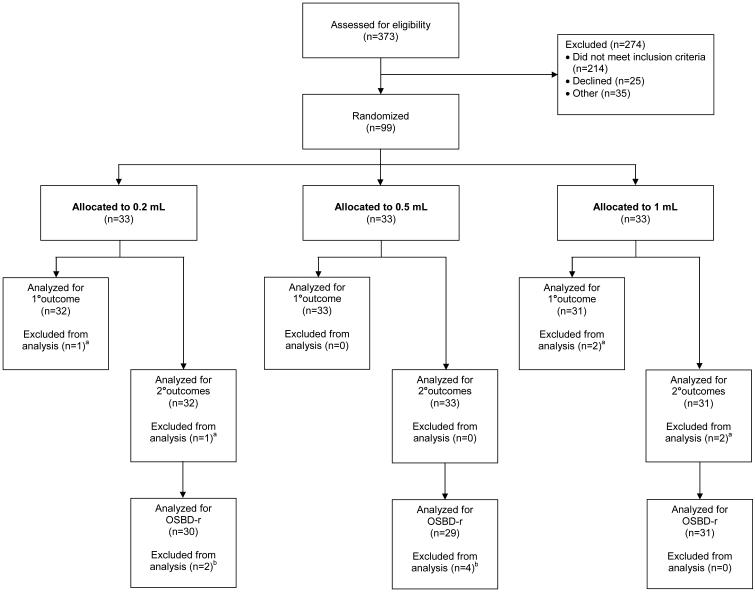
Methods: We conducted a randomized, single-blinded, 3-arm, superiority clinical trial. Children aged 1 to 7 years and undergoing laceration repair requiring 0.5 mg/kg intranasal midazolam (5 mg/mL) were block-randomized to receive midazolam using 1 of 3 volumes of administration: 0.2, 0.5, or 1 mL. Procedures were videotaped, with outcome assessors blinded to volume of administration. Primary outcome was time to onset of minimal sedation (ie, score of 1 on the University of Michigan Sedation Scale). Secondary outcomes included procedural distress, time to procedure start, deepest level of sedation achieved, adverse events, and clinician and caregiver satisfaction.
Results: Ninety-nine children were enrolled; 96 were analyzed for the primary outcome and secondary outcomes, except for the outcome of procedural distress, for which only 90 were analyzed. Time to onset of minimal sedation for each escalating volume of administration was 4.7 minutes (95% confidence interval [CI] 3.8 to 5.4 minutes), 4.3 minutes (95% CI 3.9 to 4.9 minutes), and 5.2 minutes (95% CI 4.6 to 7.0 minutes), respectively. There were no differences in secondary outcomes except for clinician satisfaction with ease of administration: fewer clinicians were satisfied when using a volume of administration of 0.2 mL.
Conclusion: There was a slightly shorter time to onset of minimal sedation when a volume of administration of 0.5 mL was used compared with 1 mL, but all 3 volumes of administration produced comparable clinical outcomes. Fewer clinicians were satisfied with ease of administration with a volume of administration of 0.2 mL.
Copyright © 2016 American College of Emergency Physicians. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Wolfe TR, Braude DA. Intranasal medication delivery for children: a brief review and update. Pediatrics. 2010;126(3):532–537. doi:10.1542/peds.2010-0616. - PubMed
-
- Yealy DM, Ellis JH, Hobbs GD, Moscati RM. Intranasal midazolam as a sedative for children during laceration repair. Am J Emerg Med. 1992;10(6):584–587. - PubMed
-
- Pires A, Fortuna A, Alves G, Falcão A. Intranasal drug delivery: how, why and what for? Journal of Pharmacy & Pharmaceutical Sciences. 2009;12(3):288–311. - PubMed
-
- Tsze DS, Steele DW, Machan JT, Akhlaghi F, Linakis JG. Intranasal ketamine for procedural sedation in pediatric laceration repair: a preliminary report. Pediatr Emerg Care. 2012;28(8):767–770. doi:10.1097/PEC.0b013e3182624935. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
