

Maternal Deaths From Suicide and Overdose in Colorado, 2004-2012
- PMID: 27824771
- PMCID: PMC5121076
- DOI: 10.1097/AOG.0000000000001695
Maternal Deaths From Suicide and Overdose in Colorado, 2004-2012
Abstract
Objective: To ascertain demographic and clinical characteristics of maternal deaths from self-harm (accidental overdose or suicide) to identify opportunities for prevention.
Methods: We report a case series of pregnancy-associated deaths resulting from self-harm in the state of Colorado between 2004 and 2012. Self-harm deaths were identified from several sources, including death certificates. Birth and death certificates along with coroner, prenatal care, and delivery hospitalization records were abstracted. Descriptive analyses were performed. For context, we describe demographic characteristics of women with a maternal death from self-harm and all women with live births in Colorado.
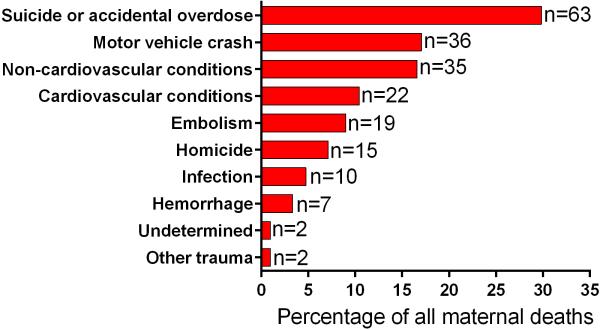
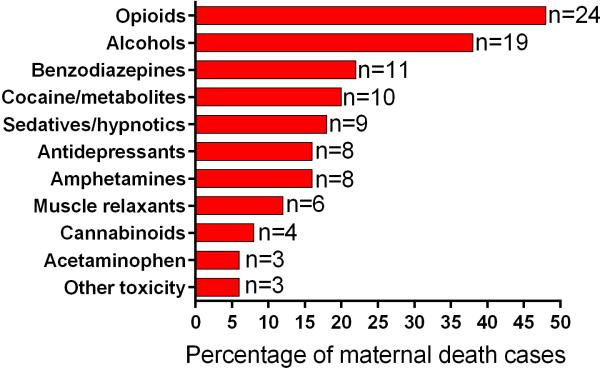
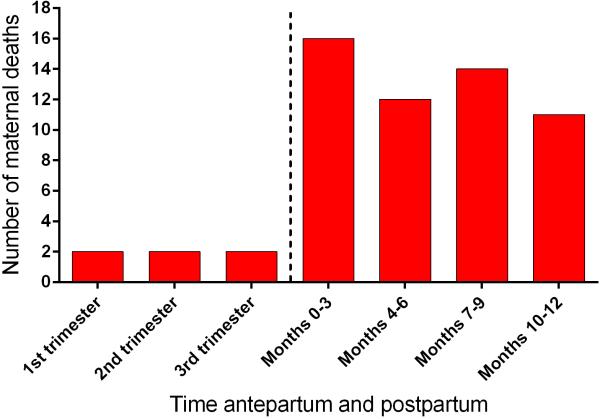
Results: Among the 211 total maternal deaths in Colorado over the study interval, 30% (n=63) resulted from self-harm. The pregnancy-associated death ratio from overdose was 5.0 (95% confidence interval [CI] 3.4-7.2) per 100,000 live births and from suicide 4.6 (95% CI 3.0-6.6) per 100,000 live births. Detailed records were obtained for 94% (n=59) of women with deaths from self-harm. Deaths were equally distributed throughout the first postpartum year (mean 6.21±3.3 months postpartum) with only six maternal deaths during pregnancy. Seventeen percent (n=10) had a known substance use disorder. Prior psychiatric diagnoses were documented in 54% (n=32) and prior suicide attempts in 10% (n=6). Although half (n=27) of the women with deaths from self-harm were noted to be taking psychopharmacotherapy at conception, 48% of them discontinued the medications during pregnancy. Fifty women had toxicology testing available; pharmaceutical opioids were the most common drug identified (n=21).
Conclusion: Self-harm was the most common cause of pregnancy-associated mortality, with most deaths occurring in the postpartum period. A four-pronged educational and program building effort to include women, health care providers, health care systems, and both governments and organizations at the community and national levels may allow for a reduction in maternal deaths.
Figures
Comment in
-
Maternal Deaths From Suicide and Overdose in Colorado, 2004-2012.Obstet Gynecol. 2017 May;129(5):946. doi: 10.1097/AOG.0000000000002005. Obstet Gynecol. 2017. PMID: 28426605 No abstract available.
References
-
- Main EK, Menard MK. Maternal mortality: time for national action. Obstet. Gynecol. 2013;122(4):735–736. - PubMed
-
- D'Alton ME, Main EK, Menard MK, Levy BS. The National Partnership for Maternal Safety. Obstet. Gynecol. 2014;123(5):973–977. - PubMed
-
- Council on Patient Safety in Women's Healthcare [May 10, 2016];Maternal mental health: perinatal depression and anxiety. http://www.safehealthcareforeverywoman.org/secure/maternal-mental-health....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
