

Urgent-Start Peritoneal Dialysis and Hemodialysis in ESRD Patients: Complications and Outcomes
- PMID: 27824950
- PMCID: PMC5100934
- DOI: 10.1371/journal.pone.0166181
Urgent-Start Peritoneal Dialysis and Hemodialysis in ESRD Patients: Complications and Outcomes
Abstract
Background: Several studies have suggested that urgent-start peritoneal dialysis (PD) is a feasible alternative to hemodialysis (HD) in patients with end-stage renal disease (ESRD), but the impact of the dialysis modality on outcome, especially on short-term complications, in urgent-start dialysis has not been directly evaluated. The aim of the current study was to compare the complications and outcomes of PD and HD in urgent-start dialysis ESRD patients.
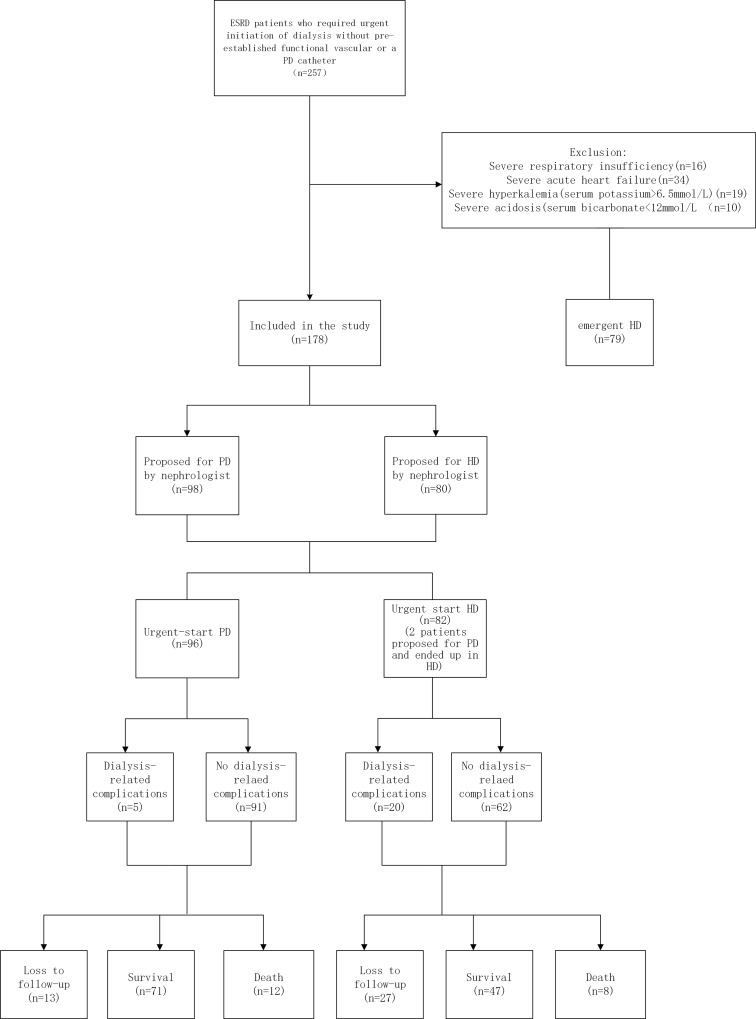
Methods: In this retrospective study, ESRD patients who initiated dialysis urgently without a pre-established functional vascular access or PD catheter at a single center from January 2013 to December 2014 were included. Patients were grouped according to their dialysis modality (PD and HD). Each patient was followed for at least 30 days after catheter insertion (until January 2016). Dialysis-related complications and patient survival were compared between the two groups.
Results: Our study enrolled 178 patients (56.2% male), of whom 96 and 82 patients were in the PD and HD groups, respectively. Compared with HD patients, PD patients had more cardiovascular disease, less heart failure, higher levels of serum potassium, hemoglobin, serum albumin, serum pre-albumin, and lower levels of brain natriuretic peptide. There were no significant differences in gender, age, use of steroids, early referral to a nephrologist, prevalence of primary renal diseases, prevalence of co-morbidities, and other laboratory characteristics between the groups. The incidence of dialysis-related complications during the first 30 days was significantly higher in HD than PD patients. HD patients had a significantly higher probability of bacteremia compared to PD patients. HD was an independent predictor of short-term (30-day) dialysis-related complications. There was no significant difference between PD and HD patients with respect to patient survival rate.
Conclusion: In an experienced center, PD is a safe and feasible dialysis alternative to HD for ESRD patients with an urgent need for dialysis.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- United States Renal Data System. USRDS 2014 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. Vol. 1. Ch. 1: CKD in the general population. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2014.
-
- United States Renal Data System. USRDS 2014 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. Vol. 2. Ch. 1: Incidence, prevalence, patient characteristics, and treatment modalities. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2014.
-
- United States Renal Data System. USRDS 2015 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. Vol. 2. Ch. 4: Vascular access. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2015.
-
- Povlsen JV, Ivarsen P. How to start the late referred ESRD patient urgently on chronic APD. Nephrol Dial Trans. 2006;21: 56–59. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
