

Genetic variants associated with gastrointestinal symptoms in Fabry disease
- PMID: 27825144
- PMCID: PMC5349883
- DOI: 10.18632/oncotarget.13135
Genetic variants associated with gastrointestinal symptoms in Fabry disease
Abstract
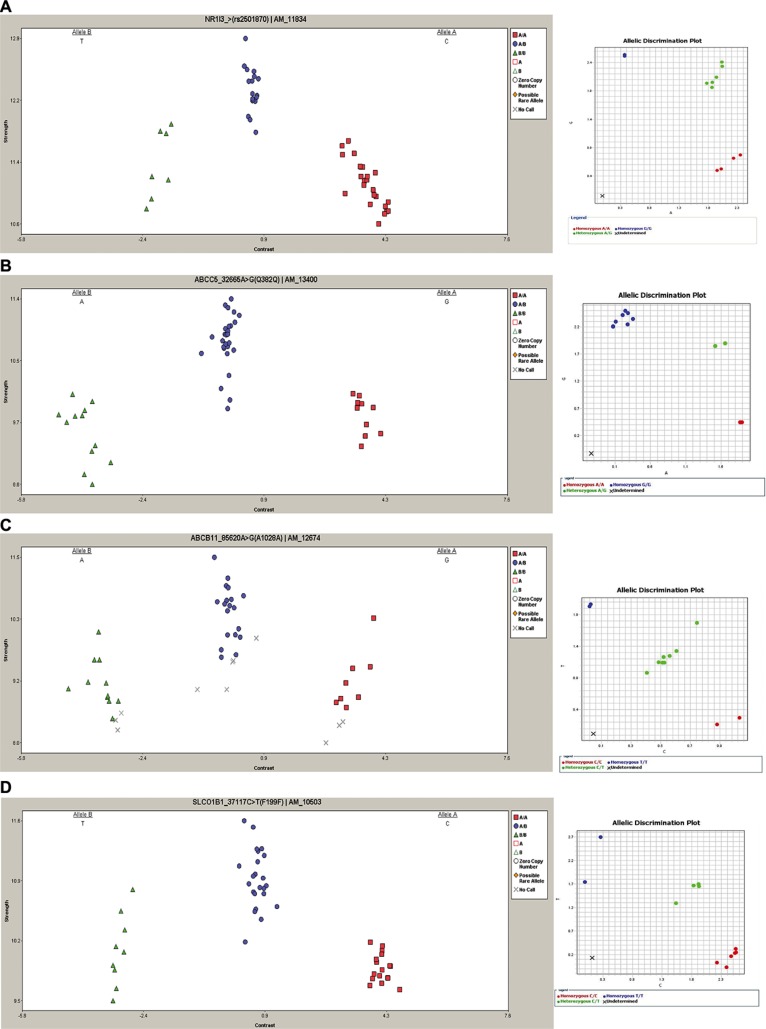
Gastrointestinal symptoms (GIS) are often among the earliest presenting events in Fabry disease (FD), an X-linked lysosomal disorder caused by the deficiency of α-galactosidase A. Despite recent advances in clinical and molecular characterization of FD, the pathophysiology of the GIS is still poorly understood. To shed light either on differential clinical presentation or on intervariability of GIS in FD, we genotyped 1936 genetic markers across 231 genes that encode for drug-metabolizing enzymes and drug transport proteins in 49 FD patients, using the DMET Plus platform. All nine single nucleotide polymorphisms (SNPs) mapped within four genes showed statistically significant differences in genotype frequencies between FD patients who experienced GIS and patients without GIS: ABCB11 (odd ratio (OR) = 18.07, P = 0,0019; OR = 8.21, P = 0,0083; OR=8.21, P = 0,0083; OR = 8.21, P = 0,0083),SLCO1B1 (OR = 9.23, P = 0,0065; OR = 5.08, P = 0,0289; OR = 8.21, P = 0,0083), NR1I3 (OR = 5.40, P = 0,0191) and ABCC5 (OR = 14.44, P = 0,0060). This is the first study that investigates the relationships between genetic heterogeneity in drug absorption, distribution, metabolism and excretion (ADME) related genes and GIS in FD. Our findings provide a novel genetic variant framework which warrants further investigation for precision medicine in FD.
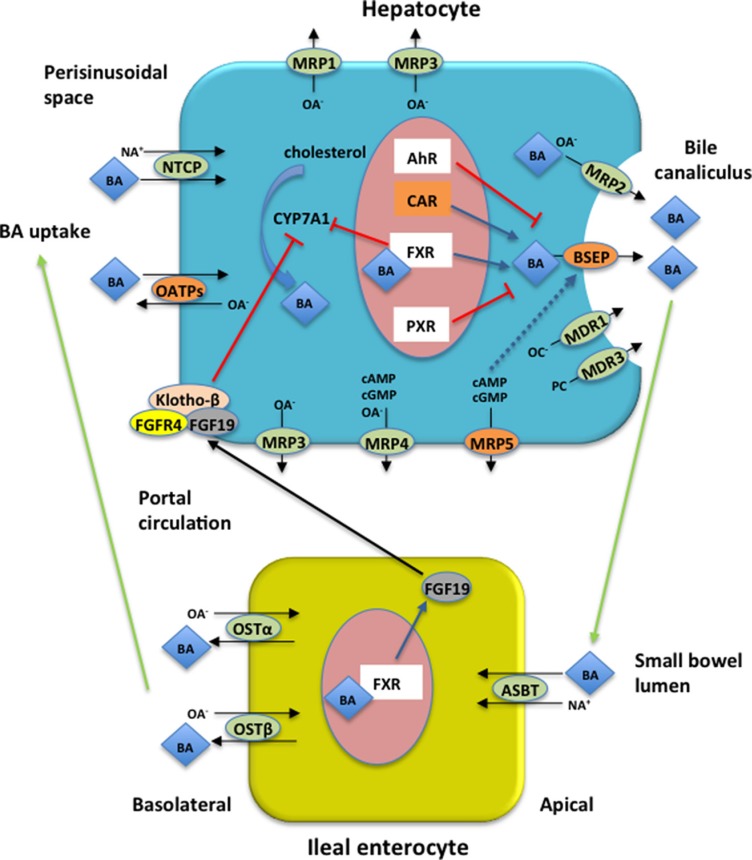
Keywords: DMET; Fabry disease; bile acids; gastrointestinal symptoms; genetic polymorphisms.
Conflict of interest statement
The authors declare no conflicts of interest
Figures
References
-
- Tuttolomondo A, Pecoraro R, Simonetta I, Miceli S, Pinto A, Licata G. Anderson-Fabry disease: a multiorgan disease. Curr Pharm Des. 2013;19:5974–5996. - PubMed
-
- Desnick RG JY, Eng CM. α-Galactosidase A deficiency: Fabry disease. In: Graw-Hill M, editor. The Metabolic and Molecular Bases of Inherited Disease. New York: 2001. pp. 3733–3774.
-
- Sestito S, Ceravolo F, Concolino D. Anderson-Fabry disease in children. Pharm Des. 2013;19:6037–6045. - PubMed
-
- Nakao S, Takenaka T, Maeda M, Kodama C, Tanaka A, Tahara M, Yoshida A, Kuriyama M, Hayashibe H, Sakuraba H, et al. An atypical variant of Fabry’s disease in men with left ventricular hypertrophy. N Engl J Med. 1995;333:288–293. - PubMed
-
- Nakao S, Kodama C, Takenaka T, Tanaka A, Yasumoto Y, Yoshida A, Kanzaki T, Enriquez AL, Eng CM, Tanaka H, Tei C, Desnick RJ. Fabry disease: detection of undiagnosed hemodialysis patients and identification of a “renal variant” phenotype. Kidney Int. 2003;64:801–807. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
