

Rapid antimicrobial susceptibility test for identification of new therapeutics and drug combinations against multidrug-resistant bacteria
- PMID: 27826141
- PMCID: PMC5148025
- DOI: 10.1038/emi.2016.123
Rapid antimicrobial susceptibility test for identification of new therapeutics and drug combinations against multidrug-resistant bacteria
Abstract
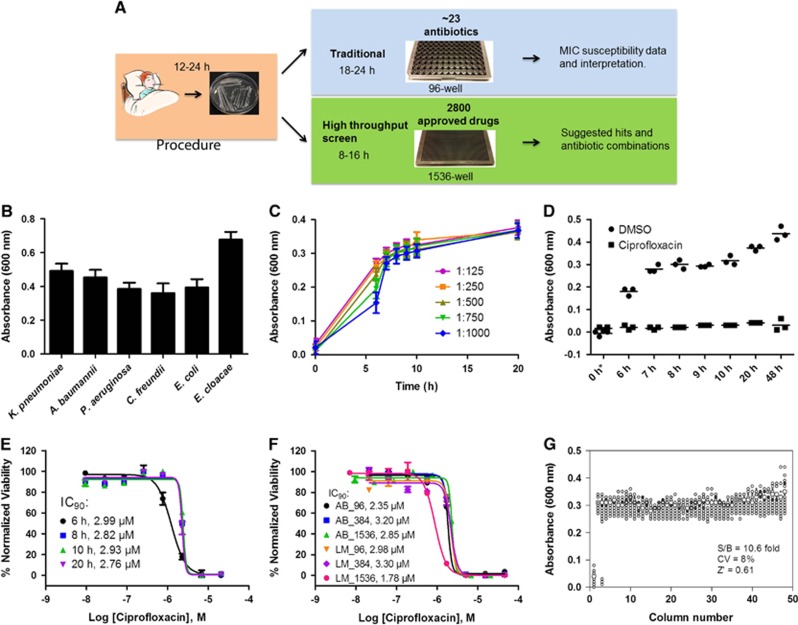
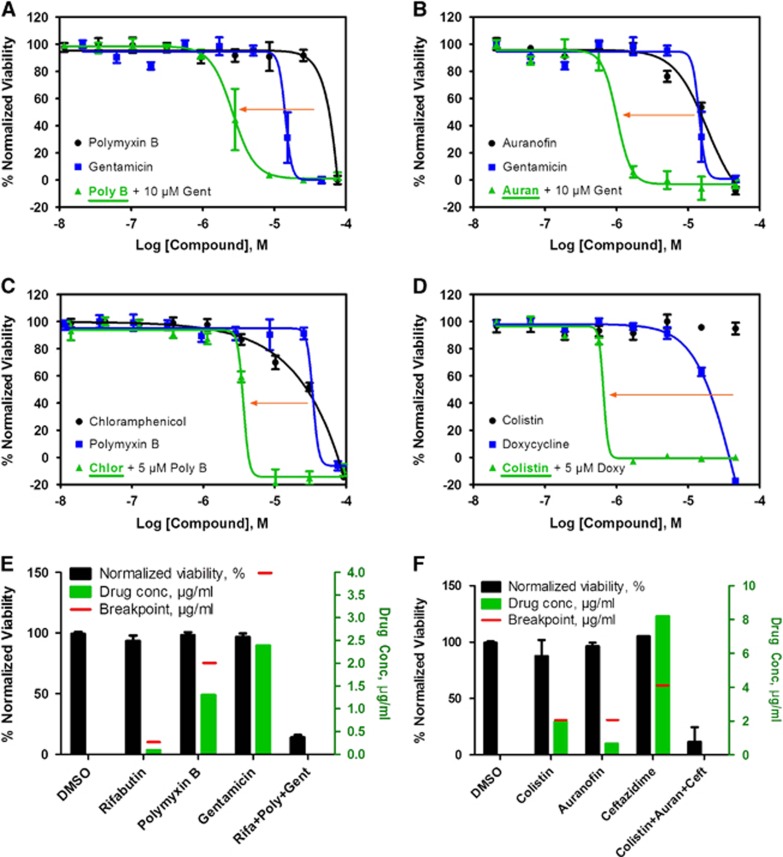
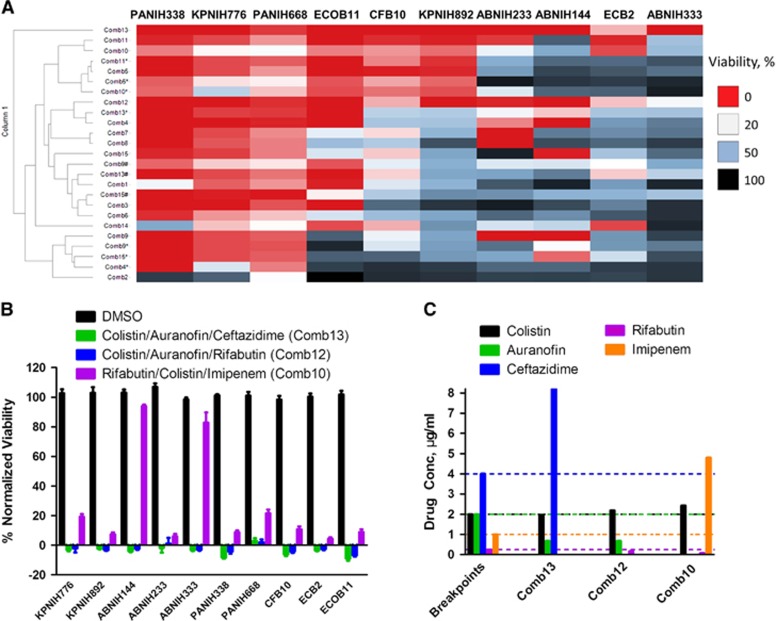
Current antimicrobial susceptibility testing has limited screening capability for identifying empirical antibiotic combinations to treat severe bacterial infections with multidrug-resistant (MDR) organisms. We developed a new antimicrobial susceptibility assay using automated ultra-high-throughput screen technology in combination with a simple bacterial growth assay. A rapid screening of 5170 approved drugs and other compounds identified 25 compounds with activities against MDR Klebsiella pneumoniae. To further improve the efficacy and reduce the effective drug concentrations, we applied a targeted drug combination approach that integrates drugs' clinical antimicrobial susceptibility breakpoints, achievable plasma concentrations, clinical toxicities and mechanisms of action to identify optimal drug combinations. Three sets of three-drug combinations were identified with broad-spectrum activities against 10 MDR clinical isolates including K. pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, Citrobacter freundii, Enterobacter cloacae and Escherichia coli. Colistin-auranofin-ceftazidime and colistin-auranofin-rifabutin suppressed >80% growth of all 10 MDR strains; while rifabutin-colistin-imipenem inhibited >75% of these strains except two Acinetobacter baumannii isolates. The results demonstrate this new assay has potential as a real-time method to identify new drugs and effective drug combinations to combat severe clinical infections with MDR organisms.
Figures


References
-
- Centers for Disease Control and Prevention. Antibiotic resistance threats in the United States, 2013. Atlanta, GA: CDC, 2016; Available at http://www.cdc.gov/drugresistance/threat-report-2013/ (accessed on 15 June 2016).
-
- Levy SB, Marshall B. Antibacterial resistance worldwide: causes, challenges and responses. Nat Med 2004 Dec; 10 (12 Suppl): S122–S129. - PubMed
-
- Jorgensen JH, Ferraro MJ. Antimicrobial susceptibility testing: a review of general principles and contemporary practices. Clin Infect Dis 2009; 149: 1749–1755. - PubMed
-
- Poulikakos P, Tansarli GS, Falagas ME. Combination antibiotic treatment versus monotherapy for multidrug-resistant, extensively drug-resistant, and pandrug-resistant Acinetobacter infections: a systematic review. Eur J Clin Microbiol Infect Dis 2014; 33: 1675–1685. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical