

Minimally invasive esophagectomy versus open esophagectomy for esophageal cancer: a meta-analysis
- PMID: 27826201
- PMCID: PMC5096744
- DOI: 10.2147/OTT.S112105
Minimally invasive esophagectomy versus open esophagectomy for esophageal cancer: a meta-analysis
Abstract
Background and objectives: The safety and effectiveness of minimally invasive esophagectomy (MIE) in comparison with the open esophagectomy (OE) remain uncertain in esophageal cancer treatment. The purpose of this meta-analysis is to compare the outcomes of the two surgical modalities.
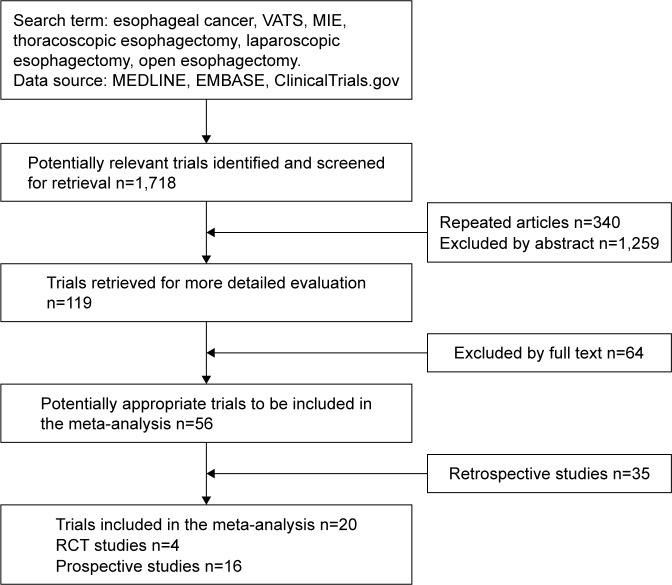
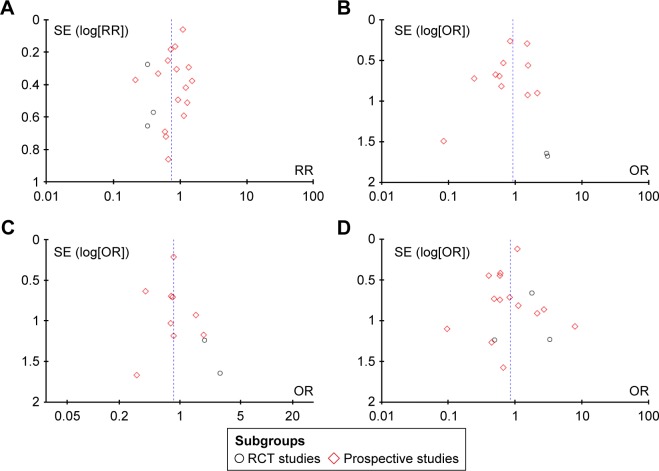
Methods: Searches were conducted in MEDLINE, EMBASE, and ClinicalTrials.gov with the following index words: "esophageal cancer", "VATS", "MIE", "thoracoscopic esophagectomy", and "open esophagectomy" for relative studies that compared the effects between MIE and OE. Random-effect models were used, and heterogeneity was assessed.
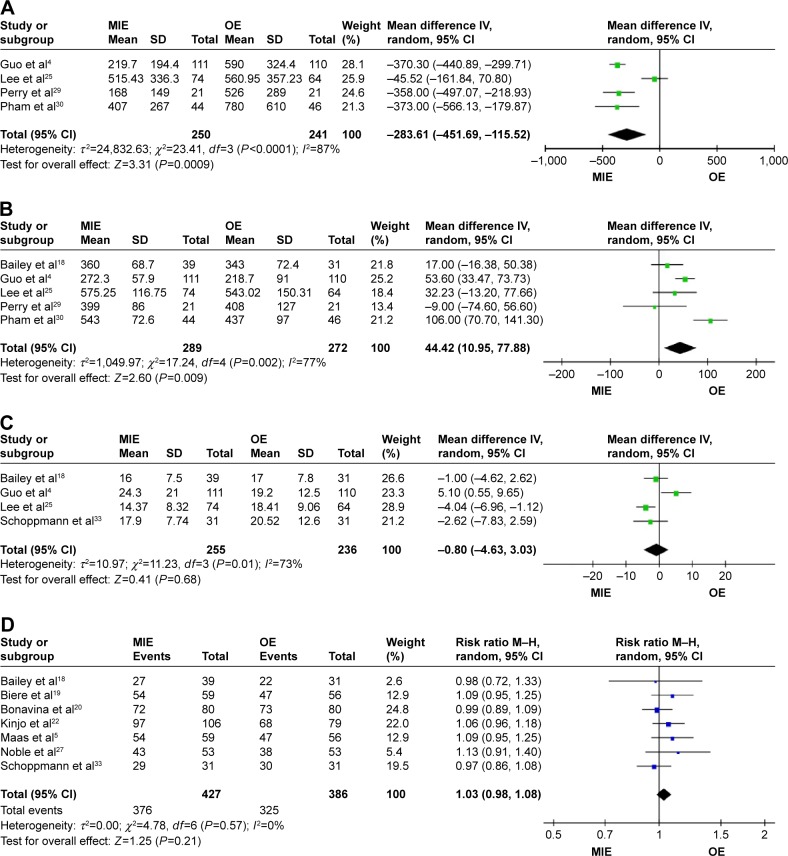
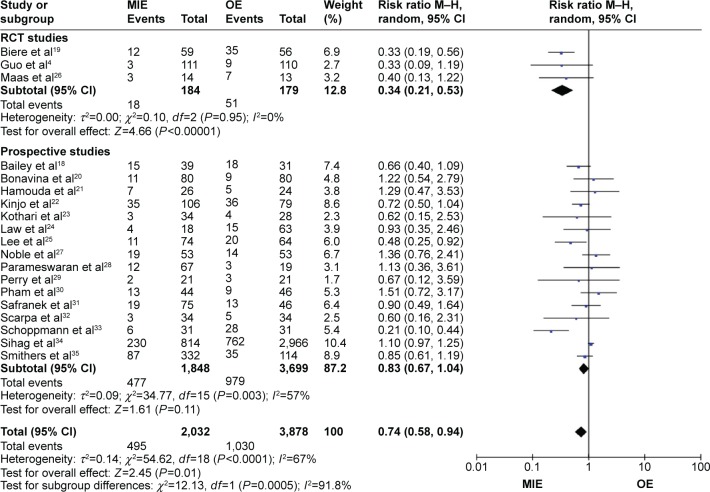
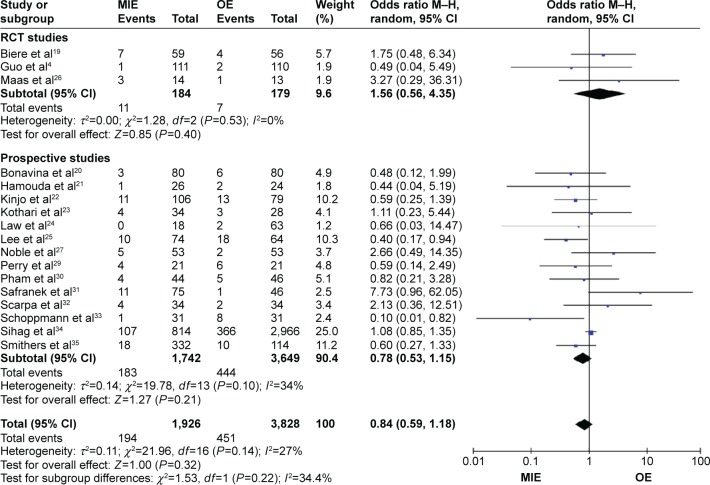
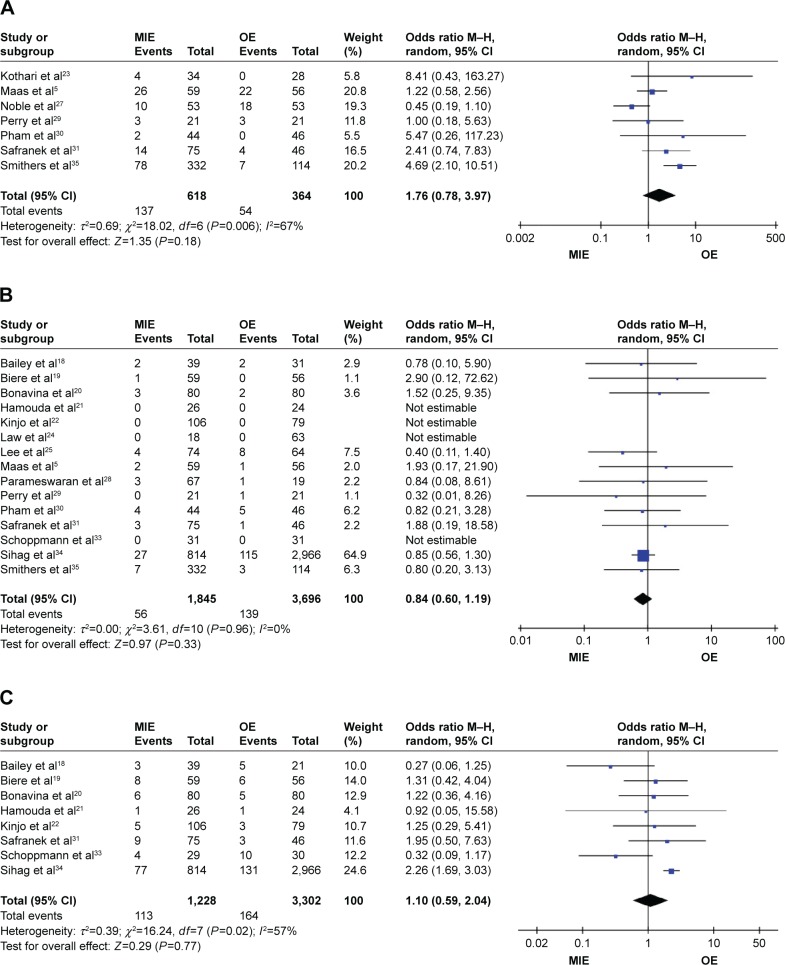
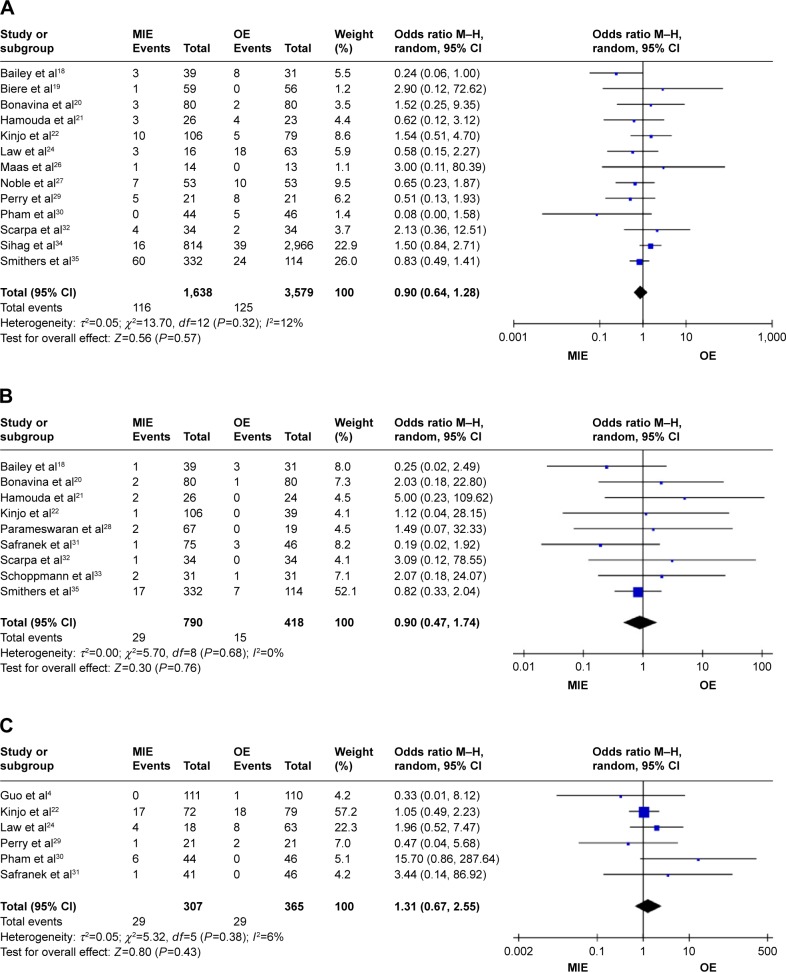
Results: A total of 20 studies were included in the analysis, consisting of four randomized controlled trials and 16 prospective studies. MIE has reduced operative blood loss (P=0.0009) but increased operation time (P=0.009) in comparison with OE. Patients get less respiratory complications (risk ratio =0.74, 95% CI =0.58-0.94, P=0.01) and better overall survival (hazard ratio =0.54, 95% CI =0.42-0.70, P<0.00001) in the MIE group than the OE group. No statistical difference was observed between the two groups in terms of lymph node harvest, R0 resection, and other major complications.
Conclusion: MIE is a better choice for esophageal cancer because patients undergoing MIE may benefit from reduced blood loss, less respiratory complications, and also improved overall survival condition compared with OE. However, more randomized controlled trials are still needed to verify these differences.
Keywords: laparoscopic esophagectomy; postoperative prognosis; thoracoscopic esophagectomy.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures

References
-
- DeSantis CE, Lin CC, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2014. CA Cancer J Clin. 2014;64(4):252–271. - PubMed
-
- Jamieson GG, Mathew G, Ludemann R, et al. Postoperative mortality following oesophagectomy and problem in reporting its rate. Br J Surg. 2004;91(8):943–947. - PubMed
-
- Cuschieri A, Shimi S, Banting S. Endoscopic oesophagectomy through a right thoracoscopic approach. J R Coll Surg Edinb. 1992;37(1):7–11. - PubMed
-
- Guo M, Xie B, Sun X, et al. A comparative study of the therapeutic effect in two protocols: video-assisted thoracic surgery combined with laparoscopy versus right open transthoracic esophagectomy for esophageal cancer management. Chin German J Clin Oncol. 2013;12:68–71.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
