

Cardiovascular Phenotypes in Children with CKD: The 4C Study
- PMID: 27827310
- PMCID: PMC5220645
- DOI: 10.2215/CJN.01090216
Cardiovascular Phenotypes in Children with CKD: The 4C Study
Abstract
Background and objectives: Cardiovascular disease is the most important comorbidity affecting long-term survival in children with CKD.
Design, setting, participants, & measurements: The Cardiovascular Comorbidity in Children with CKD Study is a multicenter, prospective, observational study in children ages 6-17 years old with initial GFR of 10-60 ml/min per 1.73 m2. The cardiovascular status is monitored annually, and subclinical cardiovascular disease is assessed by noninvasive measurements of surrogate markers, including the left ventricular mass index, carotid intima-media thickness, and central pulse wave velocity. We here report baseline data at study entry and an explorative analysis of variables associated with surrogate markers.
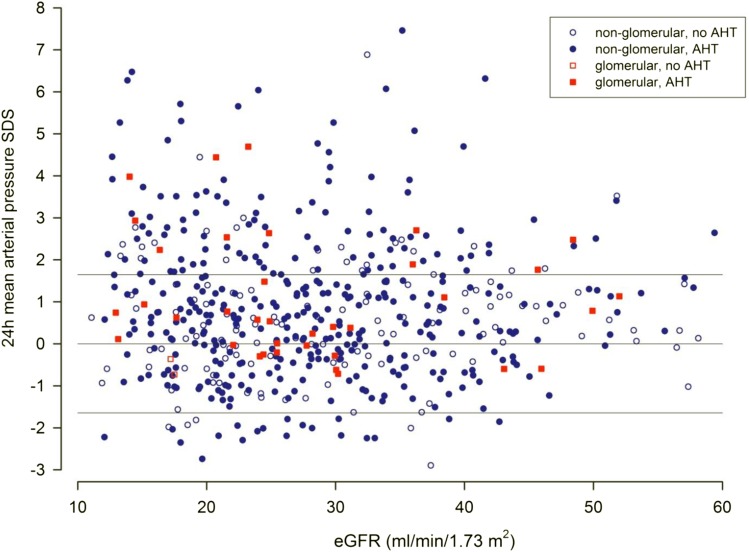
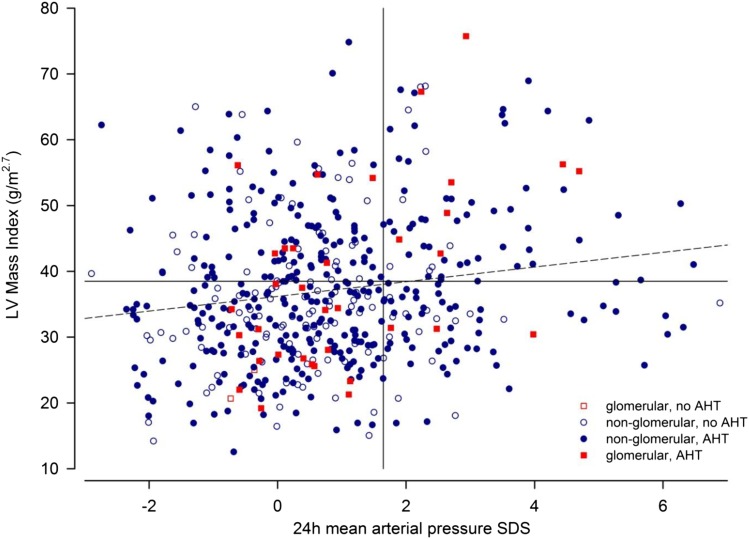
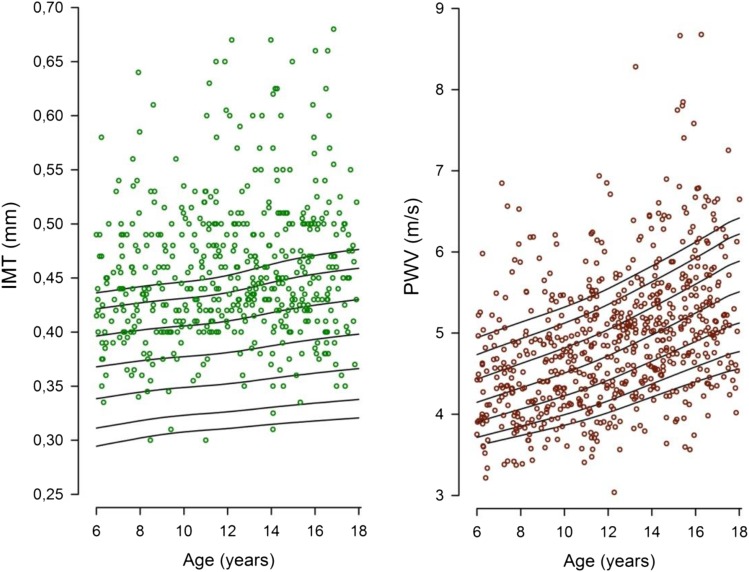
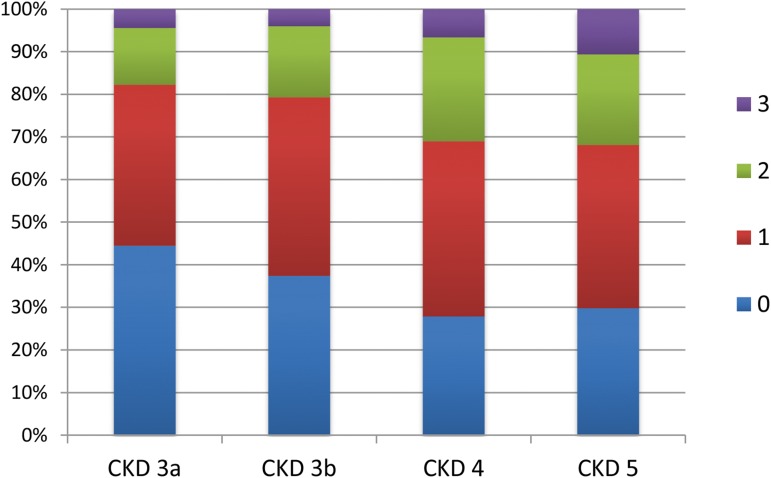
Results: A total of 737 patients were screened from October of 2009 to August of 2011 in 55 centers in 12 European countries, and baseline data were analyzed in 688 patients. Sixty-four percent had congenital anomalies of the kidney and urinary tract; 26.1% of children had uncontrolled hypertension (24-hour ambulatory BP monitoring; n=545), and the prevalence increased from 24.4% in CKD stage 3 to 47.4% in CKD stage 5. The prevalence of left ventricular hypertrophy was higher with each CKD stage, from 10.6% in CKD stage 3a to 48% in CKD stage 5. Carotid intima-media thickness was elevated in 41.6%, with only 10.8% of patients displaying measurements below the 50th percentile. Pulse wave velocity was increased in 20.1%. The office systolic BP SD score was the single independent factor significantly associated with all surrogate markers of cardiovascular disease. The intermediate end point score (derived from the number of surrogate marker measurements >95th percentile) was independently associated with a diagnosis of congenital anomalies of the kidney and urinary tract, time since diagnosis of CKD, body mass index, office systolic BP, serum phosphorus, and the hemoglobin level.
Conclusions: The baseline data of this large pediatric cohort show that surrogate markers for cardiovascular disease are closely associated with systolic hypertension and stage of CKD.
Keywords: Biomarkers; Blood Pressure Monitoring, Ambulatory; Body Mass Index; Carotid Intima-Media Thickness; Child; Comorbidity; Europe; Hemoglobins; Humans; Hypertrophy, Left Ventricular; Phenotype; Phosphorus; Phosphorus, Dietary; Prevalence; Prospective Studies; Pulse Wave Analysis; Renal Insufficiency, Chronic; arteriosclerosis; blood pressure; glomerular filtration rate; hypertension; left ventricular hypertrophy; pulse wave velocity; vesico-ureteral reflux.
Copyright © 2016 by the American Society of Nephrology.
Figures
References
-
- Querfeld U, Anarat A, Bayazit AK, Bakkaloglu AS, Bilginer Y, Caliskan S, Civilibal M, Doyon A, Duzova A, Kracht D, Litwin M, Melk A, Mir S, Sözeri B, Shroff R, Zeller R, Wühl E, Schaefer F; 4C Study Group : The cardiovascular comorbidity in children with chronic kidney disease (4C) study: Objectives, design, and methodology. Clin J Am Soc Nephrol 5: 1642–1648, 2010 - PMC - PubMed
-
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents : The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 114[Suppl 4th Report]: 555–576, 2004 - PubMed
-
- Wühl E, Witte K, Soergel M, Mehls O, Schaefer F; German Working Group on Pediatric Hypertension : Distribution of 24-h ambulatory blood pressure in children: Normalized reference values and role of body dimensions. J Hypertens 20: 1995–2007, 2002 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
