

Vasculogenic mimicry in small cell lung cancer
- PMID: 27827359
- PMCID: PMC5105195
- DOI: 10.1038/ncomms13322
Vasculogenic mimicry in small cell lung cancer
Abstract
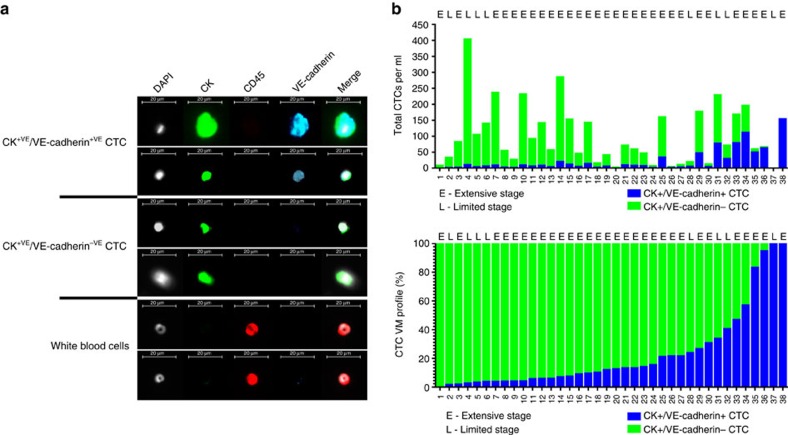
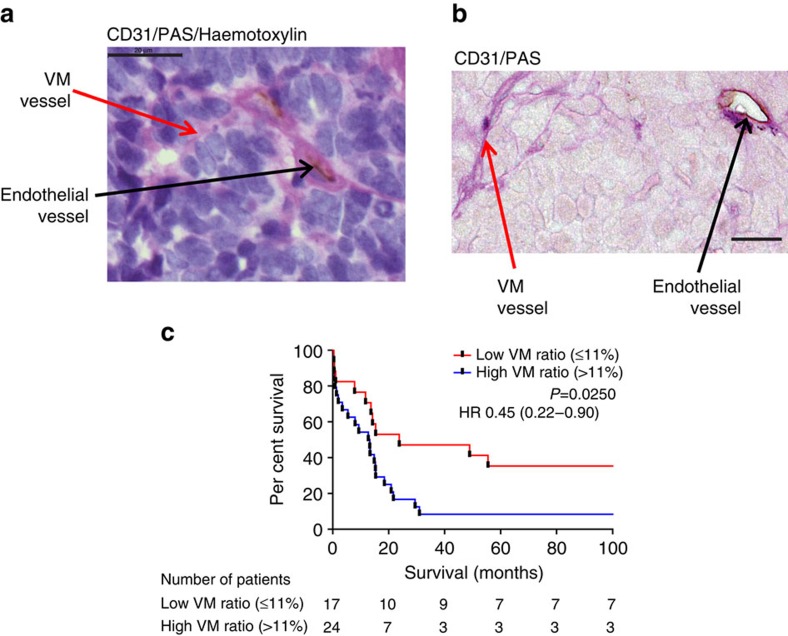
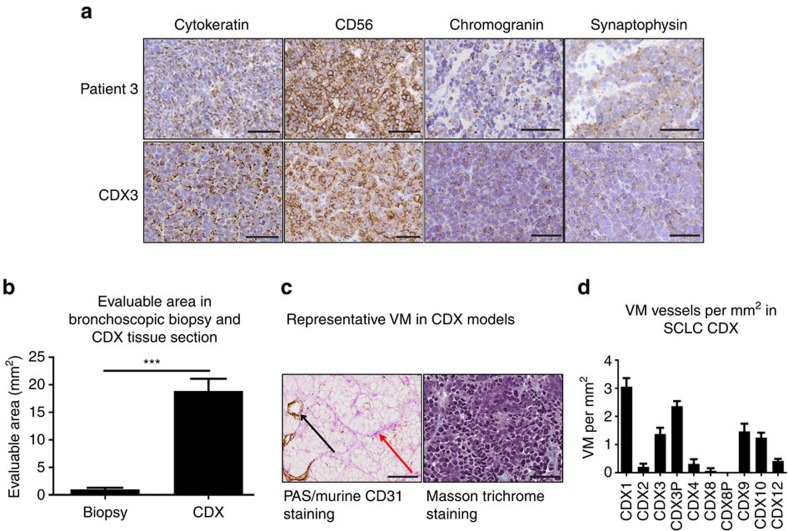
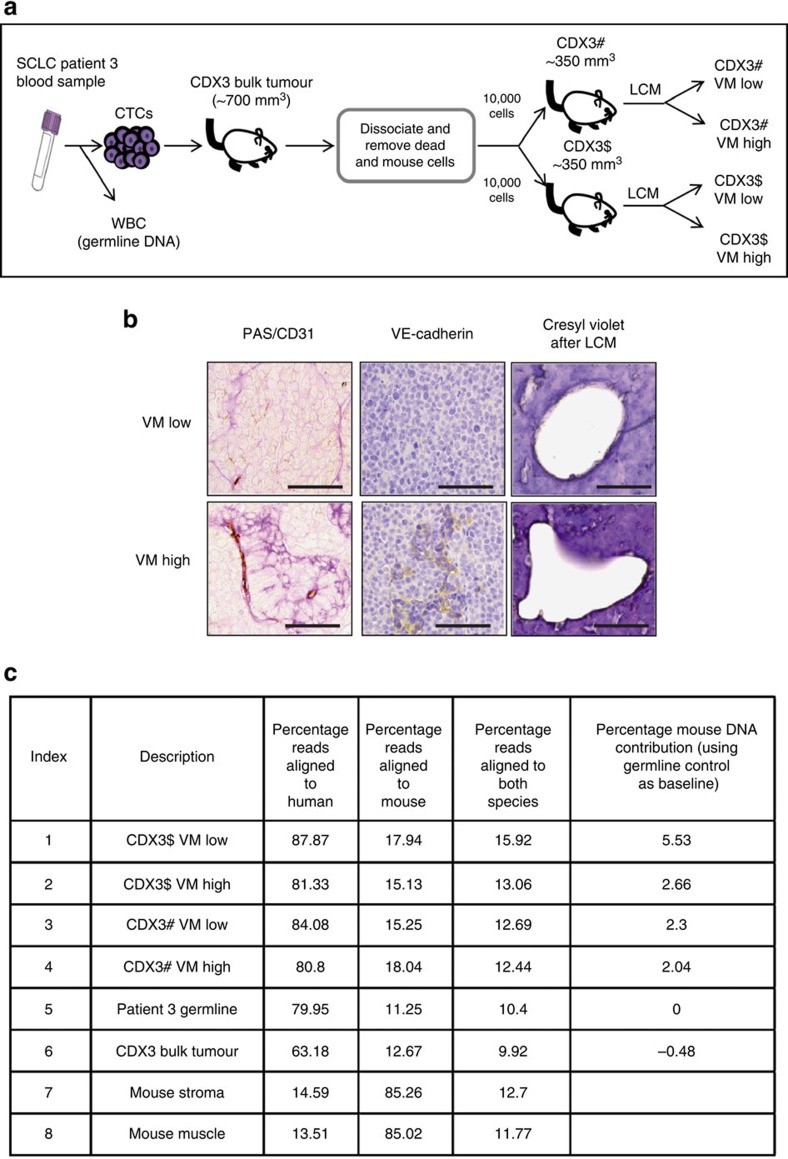
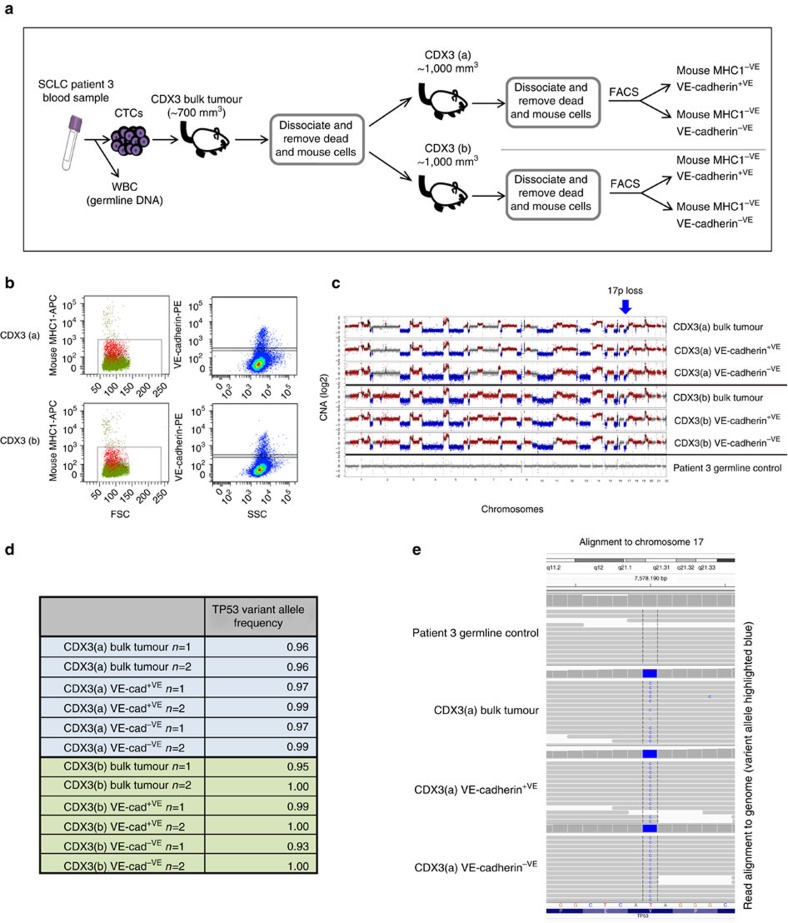
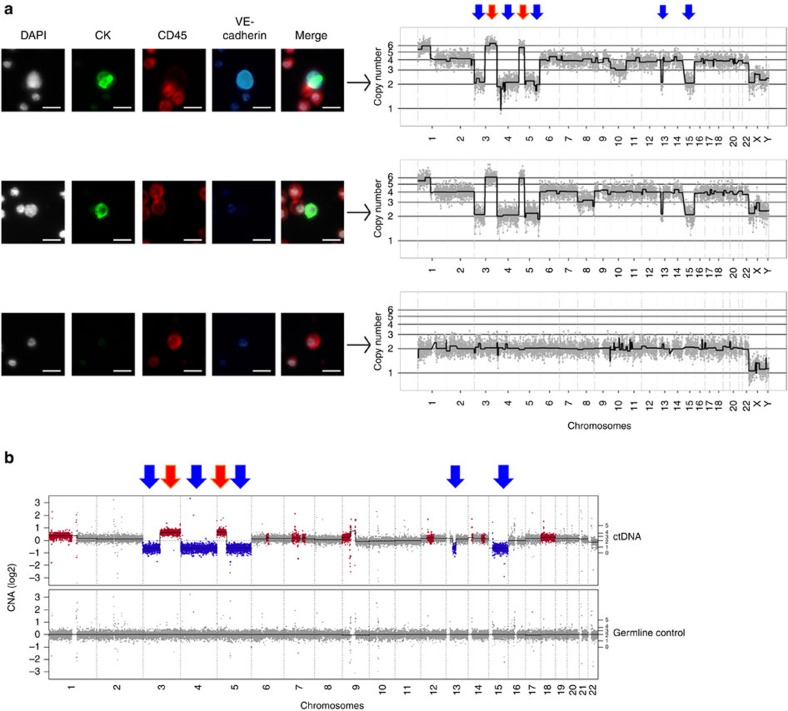
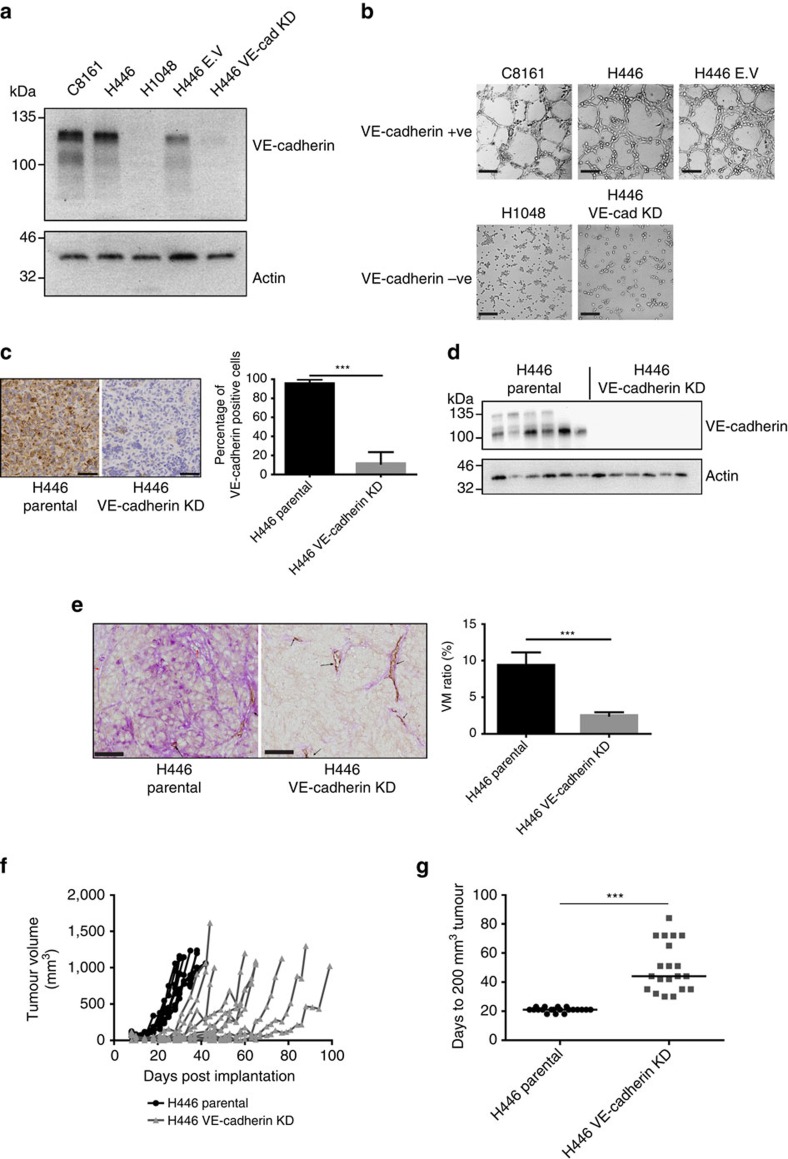
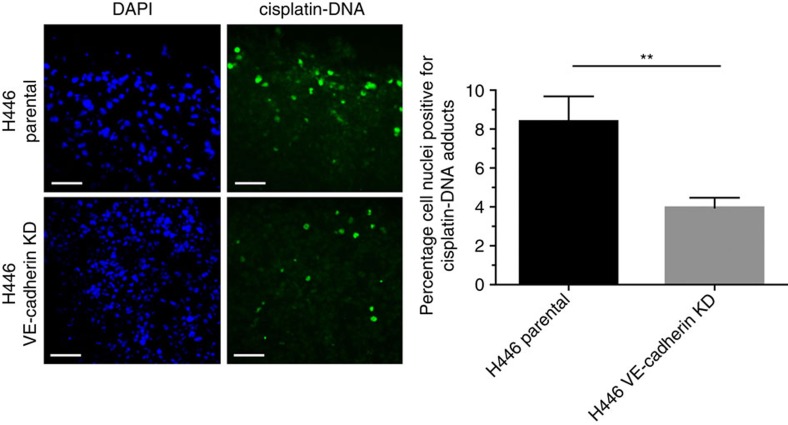
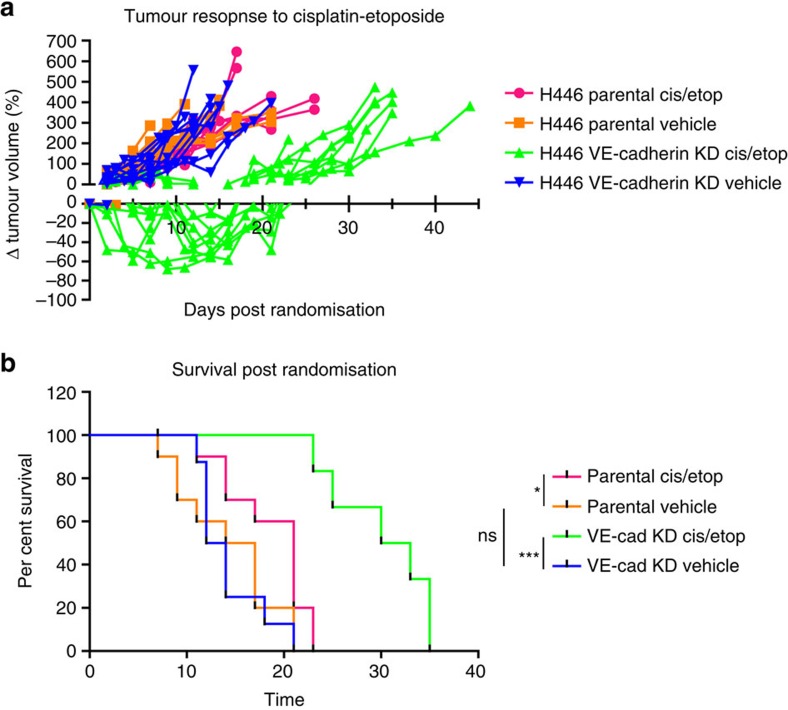
Small cell lung cancer (SCLC) is characterized by prevalent circulating tumour cells (CTCs), early metastasis and poor prognosis. We show that SCLC patients (37/38) have rare CTC subpopulations co-expressing vascular endothelial-cadherin (VE-cadherin) and cytokeratins consistent with vasculogenic mimicry (VM), a process whereby tumour cells form 'endothelial-like' vessels. Single-cell genomic analysis reveals characteristic SCLC genomic changes in both VE-cadherin-positive and -negative CTCs. Higher levels of VM are associated with worse overall survival in 41 limited-stage patients' biopsies (P<0.025). VM vessels are also observed in 9/10 CTC patient-derived explants (CDX), where molecular analysis of fractionated VE-cadherin-positive cells uncovered copy-number alterations and mutated TP53, confirming human tumour origin. VE-cadherin is required for VM in NCI-H446 SCLC xenografts, where VM decreases tumour latency and, despite increased cisplatin intra-tumour delivery, decreases cisplatin efficacy. The functional significance of VM in SCLC suggests VM regulation may provide new targets for therapeutic intervention.
Conflict of interest statement
P.K. and J.H. have ownership interest in Epic Sciences, who licensed the HD-CTC technology. The remaining authors declare no competing intersests.
Figures
References
-
- Travis W. D., Travis L. B. & Devesa S. S. Lung cancer. Cancer 75, 191–202 (1995). - PubMed
-
- Pelayo Alvarez M., Gallego Rubio O., Bonfill Cosp X. & Agra Varela Y. Chemotherapy versus best supportive care for extensive small cell lung cancer. Cochrane Database Syst Rev. 2009, CD001990 doi:10.1002/14651858.CD001990.pub2 (2009). - PubMed
-
- Morabito A. et al. Treatment of small cell lung cancer. Crit. Rev. Oncol. Hematol. 91, 257–270 (2014). - PubMed
-
- Chute J. P., Chen T., Feigal E., Simon R. & Johnson B. E. Twenty years of phase III trials for patients with extensive-stage small-cell lung cancer: perceptible progress. J. Clin. Oncol. 17, 1794–1801 (1999). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
