

Oocyte, embryo and blastocyst cryopreservation in ART: systematic review and meta-analysis comparing slow-freezing versus vitrification to produce evidence for the development of global guidance
- PMID: 27827818
- PMCID: PMC5850862
- DOI: 10.1093/humupd/dmw038
Oocyte, embryo and blastocyst cryopreservation in ART: systematic review and meta-analysis comparing slow-freezing versus vitrification to produce evidence for the development of global guidance
Abstract
Background: Successful cryopreservation of oocytes and embryos is essential not only to maximize the safety and efficacy of ovarian stimulation cycles in an IVF treatment, but also to enable fertility preservation. Two cryopreservation methods are routinely used: slow-freezing or vitrification. Slow-freezing allows for freezing to occur at a sufficiently slow rate to permit adequate cellular dehydration while minimizing intracellular ice formation. Vitrification allows the solidification of the cell(s) and of the extracellular milieu into a glass-like state without the formation of ice.
Objective and rationale: The objective of our study was to provide a systematic review and meta-analysis of clinical outcomes following slow-freezing/thawing versus vitrification/warming of oocytes and embryos and to inform the development of World Health Organization guidance on the most effective cryopreservation method.
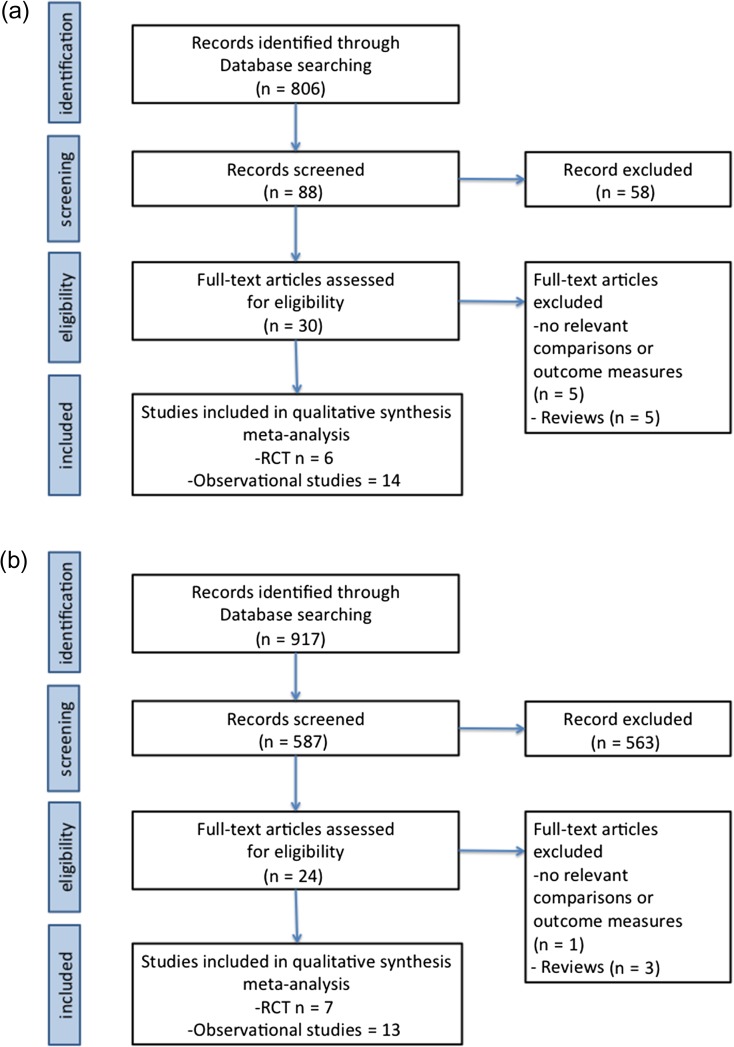
Search methods: A Medline search was performed from 1966 to 1 August 2016 using the following search terms: (Oocyte(s) [tiab] OR (Pronuclear[tiab] OR Embryo[tiab] OR Blastocyst[tiab]) AND (vitrification[tiab] OR freezing[tiab] OR freeze[tiab]) AND (pregnancy[tiab] OR birth[tiab] OR clinical[tiab]). Queries were limited to those involving humans. RCTs and cohort studies that were published in full-length were considered eligible. Each reference was reviewed for relevance and only primary evidence and relevant articles from the bibliographies of included articles were considered. References were included if they reported cryosurvival rate, clinical pregnancy rate (CPR), live-birth rate (LBR) or delivery rate for slow-frozen or vitrified human oocytes or embryos. A meta-analysis was performed using a random effects model to calculate relative risk ratios (RR) and 95% CI.
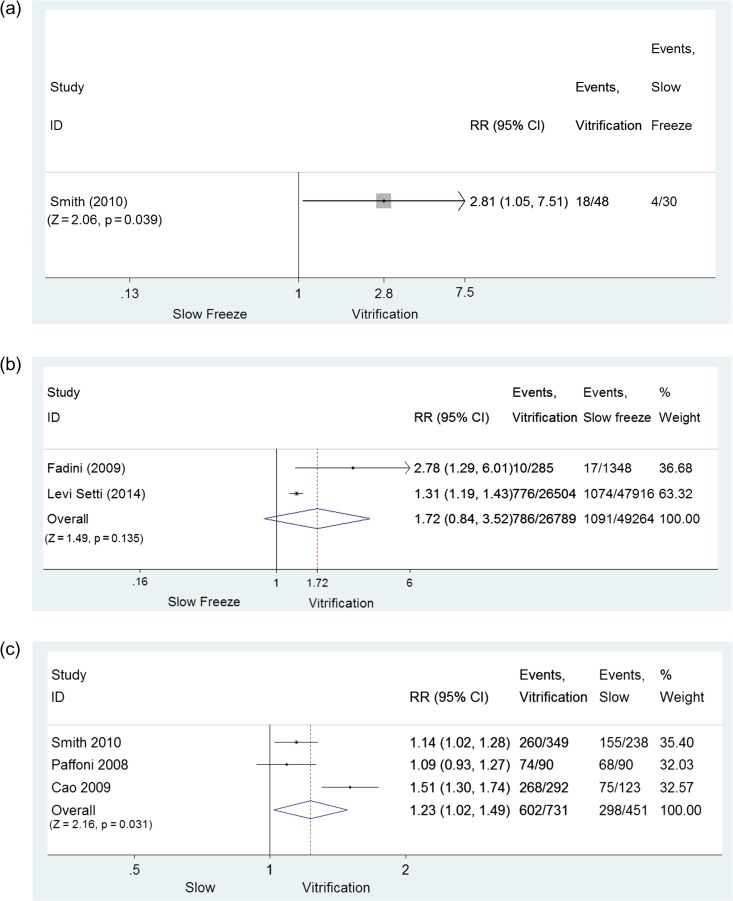
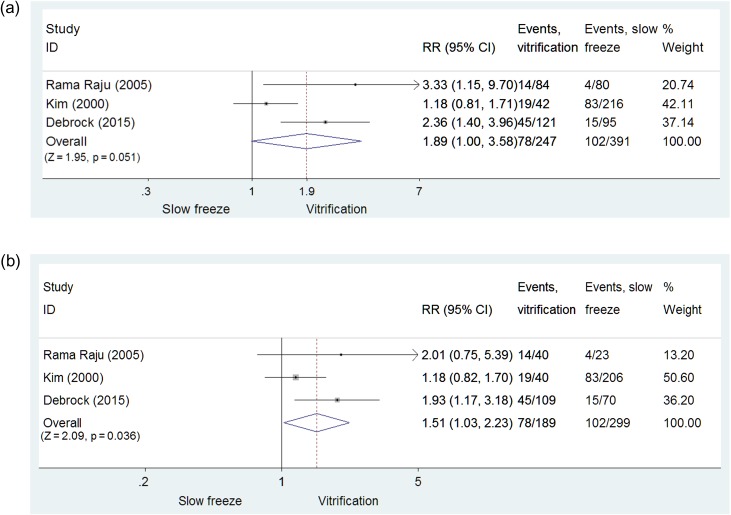
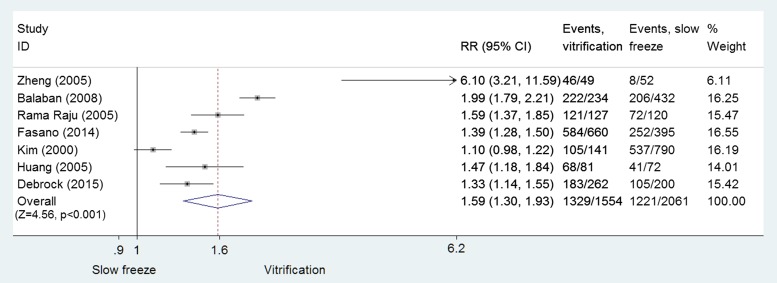
Outcomes: One RCT study comparing slow-freezing versus vitrification of oocytes was included. Vitrification was associated with increased ongoing CPR per cycle (RR = 2.81, 95% CI: 1.05-7.51; P = 0.039; 48 and 30 cycles, respectively, per transfer (RR = 1.81, 95% CI 0.71-4.67; P = 0.214; 47 and 19 transfers) and per warmed/thawed oocyte (RR = 1.14, 95% CI: 1.02-1.28; P = 0.018; 260 and 238 oocytes). One RCT comparing vitrification versus fresh oocytes was analysed. In vitrification and fresh cycles, respectively, no evidence for a difference in ongoing CPR per randomized woman (RR = 1.03, 95% CI: 0.87-1.21; P = 0.744, 300 women in each group), per cycle (RR = 1.01, 95% CI: 0.86-1.18; P = 0.934; 267 versus 259 cycles) and per oocyte utilized (RR = 1.02, 95% CI: 0.82-1.26; P = 0.873; 3286 versus 3185 oocytes) was reported. Findings were consistent with relevant cohort studies. Of the seven RCTs on embryo cryopreservation identified, three met the inclusion criteria (638 warming/thawing cycles at cleavage and blastocyst stage), none of which involved pronuclear-stage embryos. A higher CPR per cycle was noted with embryo vitrification compared with slow-freezing, though this was of borderline statistical significance (RR = 1.89, 95% CI: 1.00-3.59; P = 0.051; three RCTs; I2 = 71.9%). LBR per cycle was reported by one RCT performed with cleavage-stage embryos and was higher for vitrification (RR = 2.28; 95% CI: 1.17-4.44; P = 0.016; 216 cycles; one RCT). A secondary analysis was performed focusing on embryo cryosurvival rate. Pooled data from seven RCTs (3615 embryos) revealed a significant improvement in embryo cryosurvival following vitrification as compared with slow-freezing (RR = 1.59, 95% CI: 1.30-1.93; P < 0.001; I2 = 93%).
Wider implications: Data from available RCTs suggest that vitrification/warming is superior to slow-freezing/thawing with regard to clinical outcomes (low quality of the evidence) and cryosurvival rates (moderate quality of the evidence) for oocytes, cleavage-stage embryos and blastocysts. The results were confirmed by cohort studies. The improvements obtained with the introduction of vitrification have several important clinical implications in ART. Based on this evidence, in particular regarding cryosurvival rates, laboratories that continue to use slow-freezing should consider transitioning to the use of vitrification for cryopreservation.
Keywords: World Health Organization; blastocyst; cryopreservation; embryo; oocyte; slow freezing; vitrification.
© The Author 2016. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology.m
Figures
References
-
- AbdelHafez FF, Desai N, Abou-Setta AM, Falcone T, Goldfarb J. et al. . Slow-freezing, vitrification and ultra-rapid freezing of human embryos: a systematic review and meta-analysis. Reprod Biomed Online 2010;20:209–222. - PubMed
-
- Almodin CG, Minguetti-Camara VC, Paixao CL, Pereira PC. Embryo development and gestation using fresh and vitrified oocytes. Hum Reprod 2010;25:1192–1198. - PubMed
-
- Antinori M, Licata E, Dani G, Cerusico F, Versaci C, Antinori S. Cryotop vitrification of human oocytes results in high survival rate and healthy deliveries. Reprod Biomed Online 2007;14:72–79. - PubMed
-
- Argyle CE, Harper JC, Davies MC. Oocyte cryopreservation: where are we now. Hum Reprod Update 2016;22:440–449. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
