

Direct Measurements of Smartphone Screen-Time: Relationships with Demographics and Sleep
- PMID: 27829040
- PMCID: PMC5102460
- DOI: 10.1371/journal.pone.0165331
Direct Measurements of Smartphone Screen-Time: Relationships with Demographics and Sleep
Abstract
Background: Smartphones are increasingly integrated into everyday life, but frequency of use has not yet been objectively measured and compared to demographics, health information, and in particular, sleep quality.
Aims: The aim of this study was to characterize smartphone use by measuring screen-time directly, determine factors that are associated with increased screen-time, and to test the hypothesis that increased screen-time is associated with poor sleep.
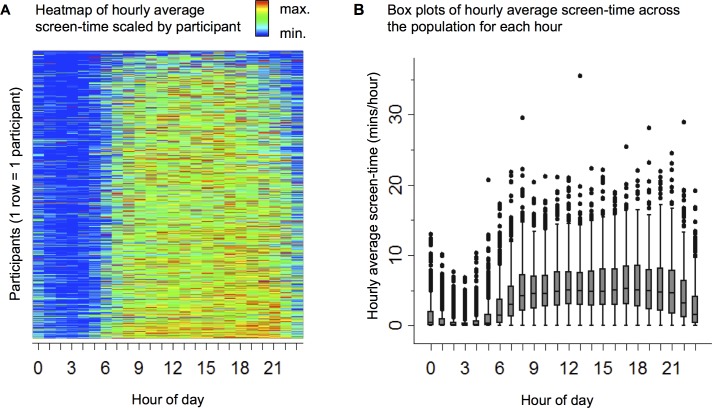
Methods: We performed a cross-sectional analysis in a subset of 653 participants enrolled in the Health eHeart Study, an internet-based longitudinal cohort study open to any interested adult (≥ 18 years). Smartphone screen-time (the number of minutes in each hour the screen was on) was measured continuously via smartphone application. For each participant, total and average screen-time were computed over 30-day windows. Average screen-time specifically during self-reported bedtime hours and sleeping period was also computed. Demographics, medical information, and sleep habits (Pittsburgh Sleep Quality Index-PSQI) were obtained by survey. Linear regression was used to obtain effect estimates.
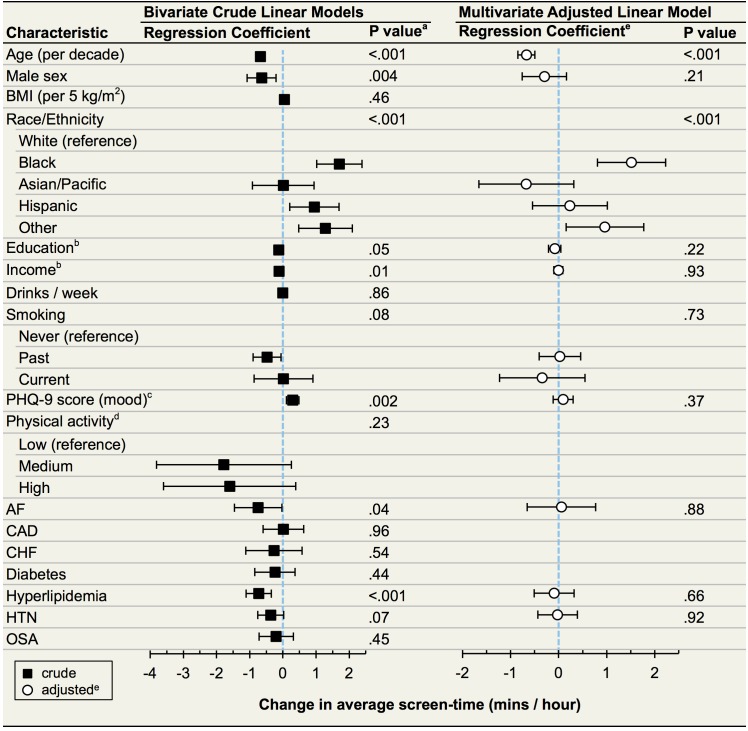
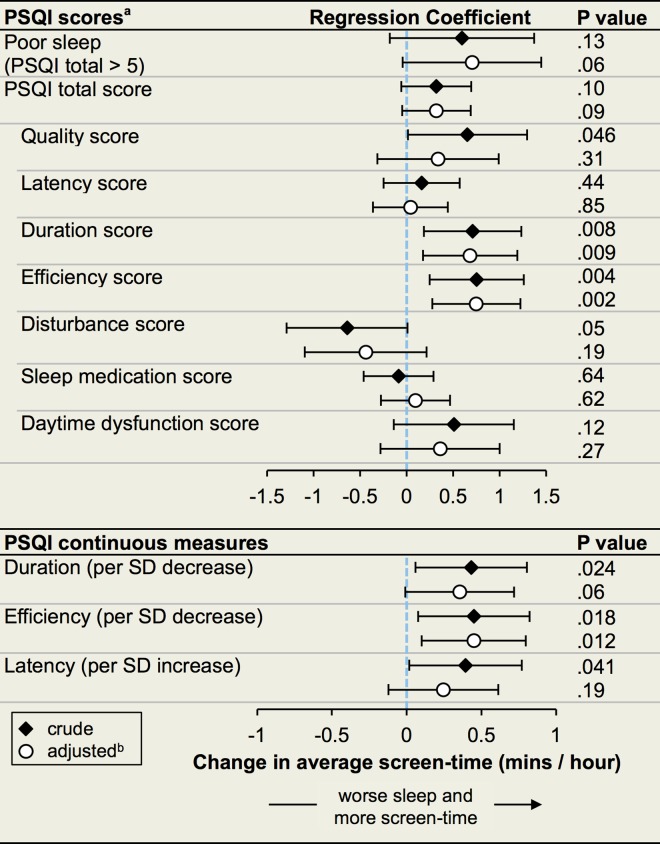
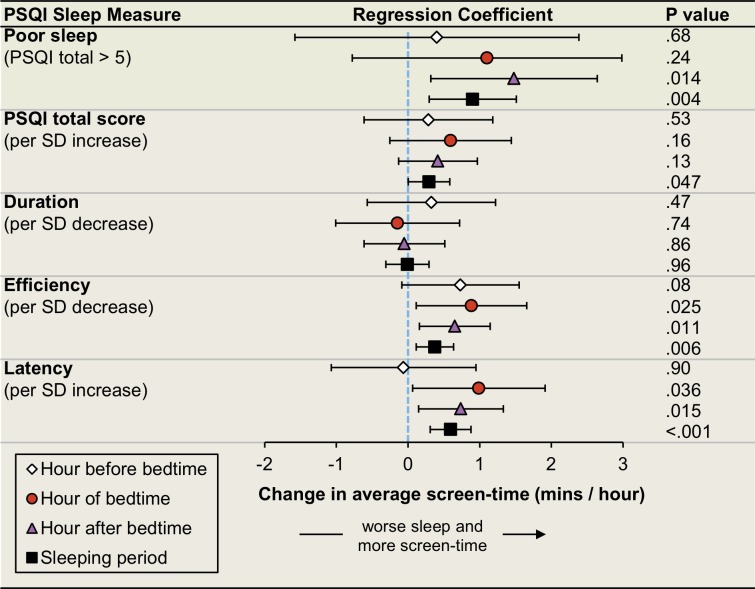
Results: Total screen-time over 30 days was a median 38.4 hours (IQR 21.4 to 61.3) and average screen-time over 30 days was a median 3.7 minutes per hour (IQR 2.2 to 5.5). Younger age, self-reported race/ethnicity of Black and "Other" were associated with longer average screen-time after adjustment for potential confounders. Longer average screen-time was associated with shorter sleep duration and worse sleep-efficiency. Longer average screen-times during bedtime and the sleeping period were associated with poor sleep quality, decreased sleep efficiency, and longer sleep onset latency.
Conclusions: These findings on actual smartphone screen-time build upon prior work based on self-report and confirm that adults spend a substantial amount of time using their smartphones. Screen-time differs across age and race, but is similar across socio-economic strata suggesting that cultural factors may drive smartphone use. Screen-time is associated with poor sleep. These findings cannot support conclusions on causation. Effect-cause remains a possibility: poor sleep may lead to increased screen-time. However, exposure to smartphone screens, particularly around bedtime, may negatively impact sleep.
Conflict of interest statement
LK and STM are employees of Ginger.io Incorporated. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures

References
-
- Smith A, Rainie L, McGeeney K, Keeter S, Duggan M. The Smartphone Difference [Internet]. Pew Research Center. 2015 [cited 2016 Mar 9]. Available from: http://www.pewinternet.org/2015/04/01/us-smartphone-use-in-2015
-
- Cappuccio FP, Cooper D, D’Elia L, Strazzullo P, Miller MA. Sleep duration predicts cardiovascular outcomes: a systematic review and meta-analysis of prospective studies. Eur Heart J [Internet]. 2011. June 2 [cited 2015 Jun 12];32(12):1484–92. Available from: http://eurheartj.oxfordjournals.org/content/32/12/1484 10.1093/eurheartj/ehr007 - DOI - PubMed
-
- Duffy JF, Czeisler C a. Effect of Light on Human Circadian Physiology. Sleep Med Clin [Internet]. 2009. June;4(2):165–77. Available from: http://linkinghub.elsevier.com/retrieve/pii/S1556407X09000058 10.1016/j.jsmc.2009.01.004 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
