

Fetal outcomes following emergency department point-of-care ultrasound for vaginal bleeding in early pregnancy
- PMID: 27829074
- PMCID: PMC4955088
Fetal outcomes following emergency department point-of-care ultrasound for vaginal bleeding in early pregnancy
Erratum in
-
Correction: Fetal outcomes following emergency department point-of-care ultrasound for vaginal bleeding in early pregnancy.Can Fam Physician. 2016 Aug;62(8):628. Can Fam Physician. 2016. PMID: 27830585 Free PMC article.
Abstract
Objective: To determine 20- and 40-week fetal outcomes following documentation of fetal cardiac activity (FCA) and intrauterine pregnancy (IUP) in women at less than 20 weeks' gestation presenting to the emergency department (ED) with vaginal bleeding.
Design: Prospective observational cohort study.
Setting: Single-centre tertiary care ED.
Participants: Pregnant women at less than 20 weeks' gestation presenting to the ED with vaginal bleeding.
Intervention: All study participants underwent ED point-of-care ultrasound (POCUS) to document IUP and FCA.
Main outcome measures: Prevalence of spontaneous abortion or pregnancy loss by 40 weeks' gestational age following ED POCUS documentation of FCA or IUP in women at less than 20 weeks' gestation.
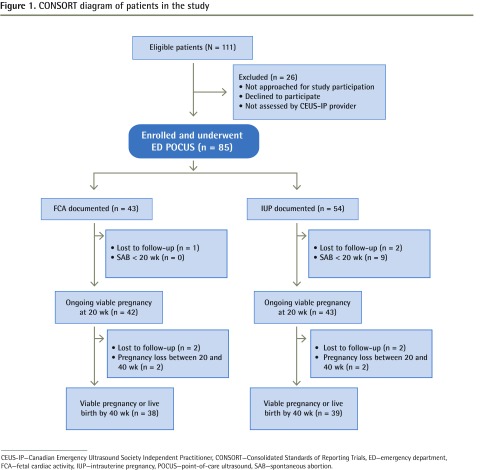
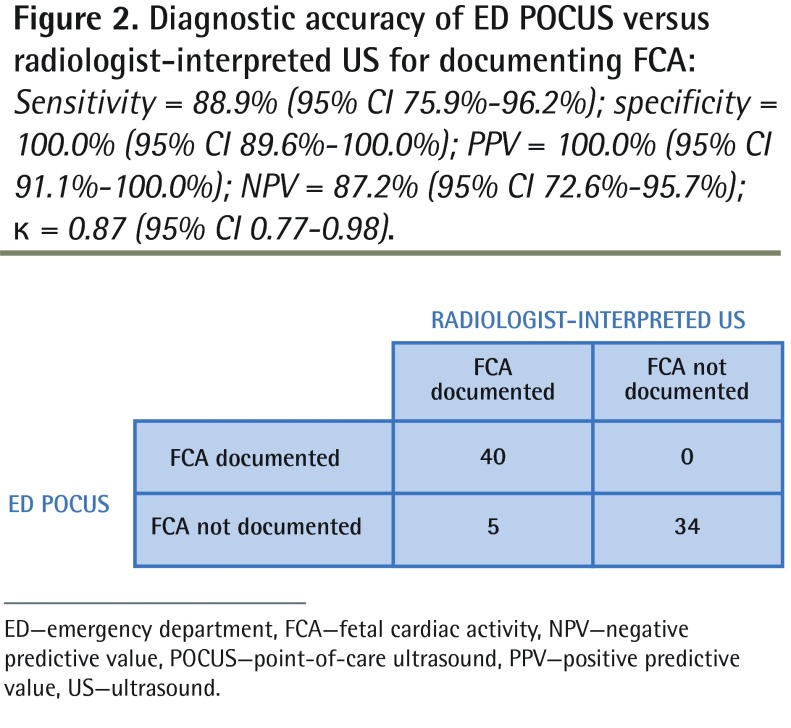
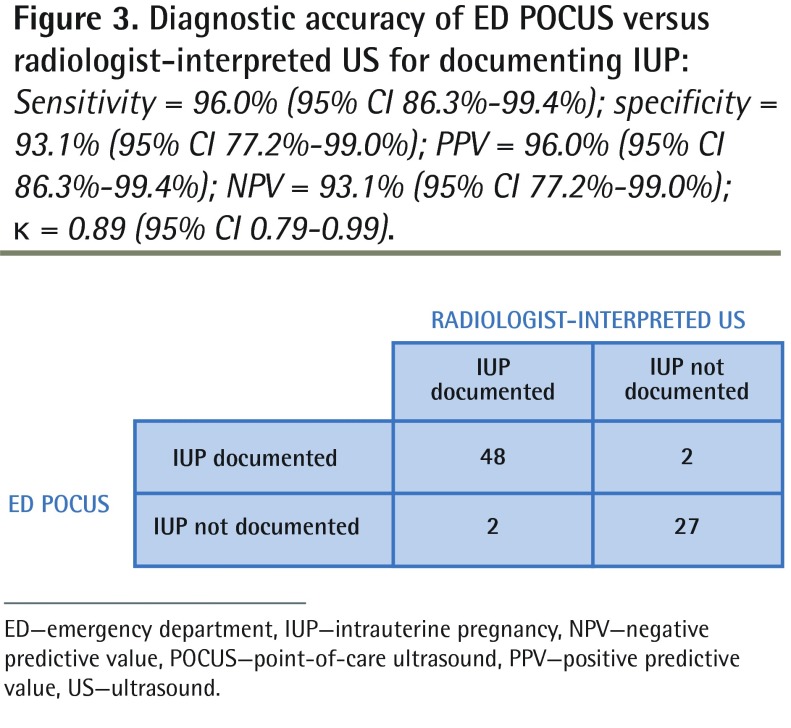
Results: A total of 85 of 111 eligible patients were enrolled; FCA and IUP were detected in 43 (50.6%) and 54 (63.5%) participants, respectively. Participants with documented FCA on ED POCUS were less likely to experience pregnancy loss than participants without documented FCA were (5.0% vs 92.7%; Δ = 87.7%; 95% CI 71.0% to 93.7%), and participants with documented IUP were less likely to experience pregnancy loss than participants without documented IUP were (22.0% vs 93.5%; Δ = 71.5%; 95% CI 52.1% to 81.9%). Compared with radiologist-interpreted ultrasound, ED POCUS had sensitivity of 88.9% (95% CI 75.9% to 96.2%) and specificity of 100.0% (95% CI 89.6% to 100.0%) for documenting FCA, and sensitivity of 96.0% (95% CI 86.3% to 99.4%) and specificity of 93.1% (95% CI 77.2% to 99.0%) for documenting IUP.
Conclusion: In this cohort of women presenting to the ED with bleeding in the first 20 weeks of pregnancy, detection of IUP and especially FCA using POCUS performed by providers certified by the Canadian Emergency Ultrasound Society was associated with ongoing viable pregnancy at 20 and 40 weeks' gestational age. These data might be useful for ED physicians counseling women with symptomatic early pregnancies about the chance of miscarriage after an episode of vaginal bleeding.
Objectif: Déterminer les incidences sur le fœtus à 20 et à 40 semaines après la documentation d’une activité cardiaque fœtale (ACF) et d’une grossesse intrautérine (GIU) chez des femmes à moins de 20 semaines de gestation qui se sont présentées à l’urgence avec des saignements vaginaux.
Conception: Étude observationnelle et prospective de cohortes.
Contexte: L’urgence d’un centre de soins tertiaires.
Participantes: Des femmes enceintes à moins de 20 semaines de gestation qui se sont présentées à l’urgence avec des saignements vaginaux.
Intervention: Toutes les participantes à l’étude ont subi une échographie au point d’intervention (EGPDI) à l’urgence pour documenter la GIU et l’ACF.
Principaux paramètres à l’étude: La prévalence d’avortements spontanés ou d’interruptions de grossesse à 40 semaines d’âge gestationnel après la documentation par EGPDI de l’ACF ou de la GIU chez des femmes à moins de 20 semaines de gestation.
Résultats: Au total, 85 des 111 femmes admissibles ont participé à l’étude; une ACF et la GIU ont été détectées respectivement chez 43 (50,6 %) et 54 (63,5 %) participantes. Les participantes chez qui une ACF a été détectée par EGPDI à l’urgence ont été moins susceptibles de vivre une interruption de grossesse que celles sans ACF documentée (5,0 % c. 92,7 %; Δ = 87,7 %; IC à 95 % de 71,0 à 93,7 %), et les participantes dont la GIU a été documentée ont été moins susceptibles de vivre une interruption de grossesse par rapport à celles dont la GIU n’a pas été documentée (22,0 % c. 93,5 %; Δ = 71,5 %; IC à 95 % de 52,1 à 81,9 %). En comparaison des échographies interprétées par un radiologiste, l’EGPDI à l’urgence avait une sensibilité de 88,9 % (IC à 95 % de 75,9 à 96,2 %) et une spécificité de 100,0 % (IC à 95 % de 89,6 à100,0 %) pour documenter l’ACF et une sensibilité de 96,0 % (IC à 95 % de 86.3 à 99.4 %) et une spécificité de 93,1 % (IC à 95 % de 77,2 à 99,0 %) pour documenter la GIU.
Conclusion: Dans cette cohorte de femmes qui se sont présentées à l’urgence avec des saignements vaginaux durant les 20 premières semaines de grossesse, la détection de la GIU et surtout de l’ACF à l’aide d’une EGPDI, effectuée par des professionnels certifiés par la Société canadienne d’échographie au département d’urgence, a été associée à une grossesse viable sans interruption à 20 et à 40 semaines d’âge gestationnel. Cette information pourrait être utile aux médecins à l’urgence pour conseiller les femmes en début de grossesse symptomatique au sujet des risques d’avortement spontané après un épisode de saignements vaginaux.
Figures
Similar articles
-
Fetal loss in symptomatic first-trimester pregnancy with documented yolk sac intrauterine pregnancy.Am J Emerg Med. 2012 Mar;30(3):399-404. doi: 10.1016/j.ajem.2010.12.021. Epub 2011 Feb 5. Am J Emerg Med. 2012. PMID: 21296521
-
Effect of Emergency Physician-Performed Point-of-Care Ultrasound and Radiology Department-Performed Ultrasound Examinations on the Emergency Department Length of Stay Among Pregnant Women at Less Than 20 Weeks' Gestation.J Ultrasound Med. 2018 Nov;37(11):2497-2505. doi: 10.1002/jum.14607. Epub 2018 Mar 25. J Ultrasound Med. 2018. PMID: 29574878 Clinical Trial.
-
Point-of-care ultrasound for evaluation of vaginal bleeding or abdominal pain in early pregnancy: Use by family physicians following focused training and certification.Can Fam Physician. 2022 Nov;68(11):e326-e332. doi: 10.46747/cfp.6811e326. Can Fam Physician. 2022. PMID: 36376040 Free PMC article.
-
Ultrasound assessment of premenopausal bleeding.Obstet Gynecol Clin North Am. 2011 Mar;38(1):115-47, viii. doi: 10.1016/j.ogc.2011.02.006. Obstet Gynecol Clin North Am. 2011. PMID: 21419330 Review.
-
Sonographic evaluation of first-trimester bleeding.Radiol Clin North Am. 2004 Mar;42(2):297-314. doi: 10.1016/j.rcl.2004.01.005. Radiol Clin North Am. 2004. PMID: 15136018 Review.
Cited by
-
Performance of single serum progesterone in the evaluation of symptomatic first-trimester pregnant patients: a systematic review and meta-analysis.CJEM. 2022 Sep;24(6):611-621. doi: 10.1007/s43678-022-00332-x. Epub 2022 Aug 3. CJEM. 2022. PMID: 35921048
-
Portable ultrasound technologies for estimating gestational age in pregnant women: a scoping review and analysis of commercially available models.BMJ Open. 2022 Nov 30;12(11):e065181. doi: 10.1136/bmjopen-2022-065181. BMJ Open. 2022. PMID: 36450429 Free PMC article.
-
Variables Associated With Favorable Obstetrical Outcomes in Early Pregnancy Bleeding in the Emergency Department.Cureus. 2024 Oct 7;16(10):e70986. doi: 10.7759/cureus.70986. eCollection 2024 Oct. Cureus. 2024. PMID: 39507153 Free PMC article.
-
Correction: Fetal outcomes following emergency department point-of-care ultrasound for vaginal bleeding in early pregnancy.Can Fam Physician. 2016 Aug;62(8):628. Can Fam Physician. 2016. PMID: 27830585 Free PMC article.
-
Point-of-care ultrasound in primary care: a systematic review of generalist performed point-of-care ultrasound in unselected populations.Ultrasound J. 2019 Nov 19;11(1):31. doi: 10.1186/s13089-019-0145-4. Ultrasound J. 2019. PMID: 31749019 Free PMC article. Review.
References
-
- College of Family Physicians of Canada . Family medicine maternity care: implications for the future. Mississauga, ON: College of Family Physicians of Canada; 2009.
-
- Barnhart KT. Clinical practice. Ectopic pregnancy. N Engl J Med. 2009;361(14):379–87. - PubMed
-
- Shih CH. Effect of emergency physician–performed pelvic sonography on length of stay in the emergency department. Ann Emerg Med. 1997;29(3):348–52. - PubMed
-
- Mallin M, Dawson M, Schroeder E, Hatch B, Jackson I, Ahern M, et al. Prospective outcomes of pregnant ED patients with documented fetal cardiac activity on ultrasound. Am J Emerg Med. 2012;30(3):472–5. Epub 2011 Feb 18. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical