

Telemedicine Technologies for Diabetes in Pregnancy: A Systematic Review and Meta-Analysis
- PMID: 27829574
- PMCID: PMC5121530
- DOI: 10.2196/jmir.6556
Telemedicine Technologies for Diabetes in Pregnancy: A Systematic Review and Meta-Analysis
Abstract
Background: Diabetes in pregnancy is a global problem. Technological innovations present exciting opportunities for novel approaches to improve clinical care delivery for gestational and other forms of diabetes in pregnancy.
Objective: To perform an updated and comprehensive systematic review and meta-analysis of the literature to determine whether telemedicine solutions offer any advantages compared with the standard care for women with diabetes in pregnancy.
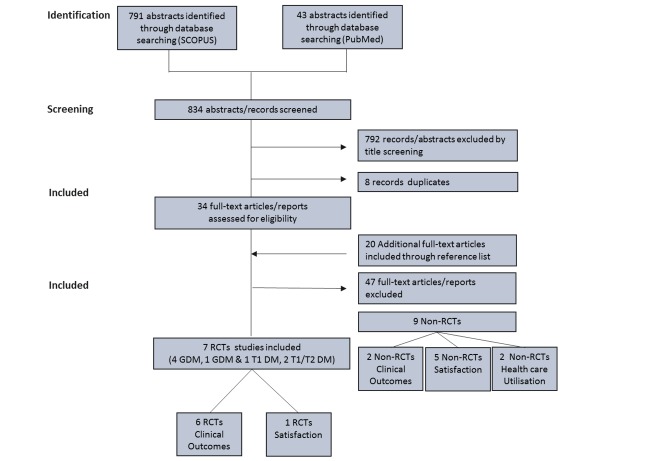
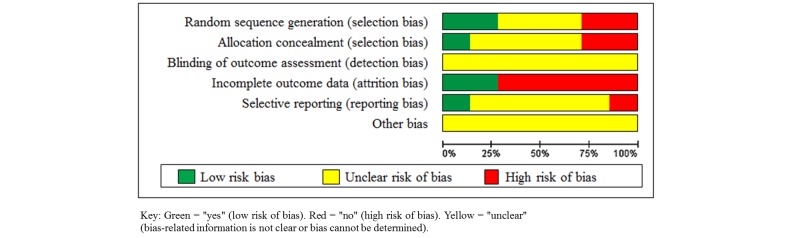
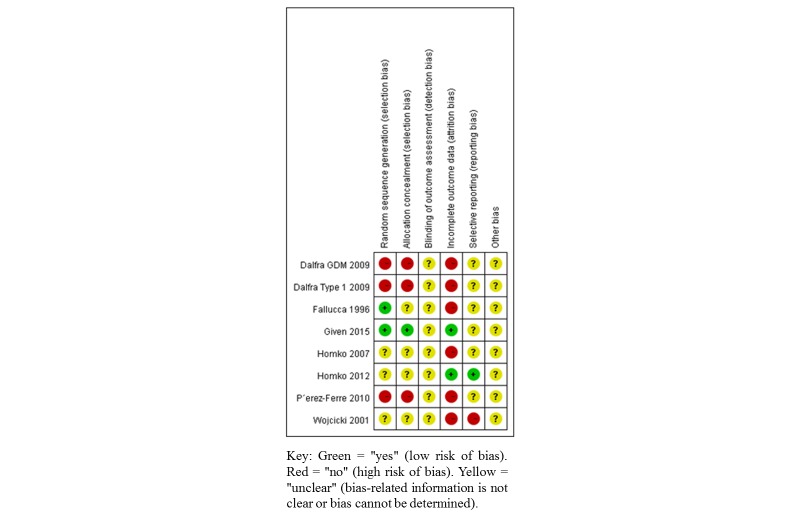
Methods: The review was developed using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework. Randomized controlled trials (RCT) in women with diabetes in pregnancy that compared telemedicine blood glucose monitoring with the standard care were identified. Searches were performed in SCOPUS and PubMed, limited to English language publications between January 2000 and January 2016. Trials that met the eligibility criteria were scored for risk of bias using the Cochrane Collaborations Risk of Bias Tool. A meta-analysis was performed using Review Manager software version 5.3 (Nordic Cochrane Centre, Cochrane Collaboration).
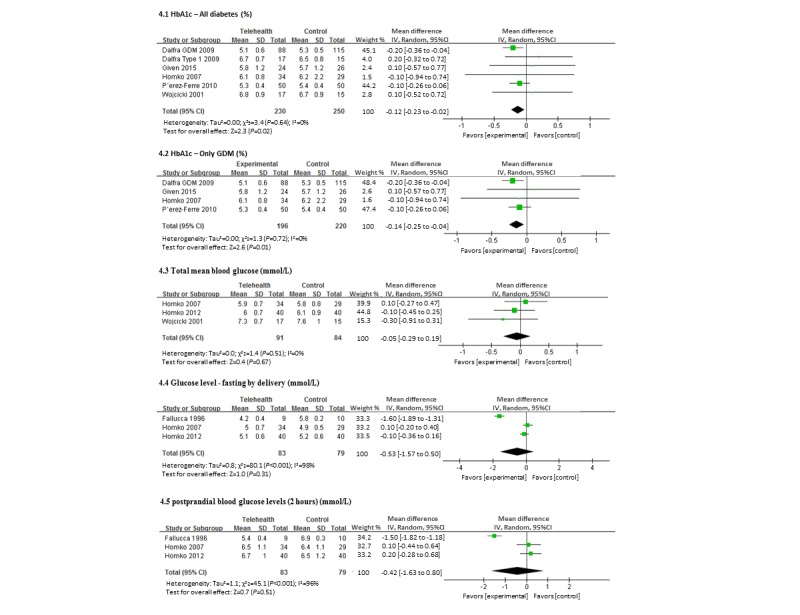
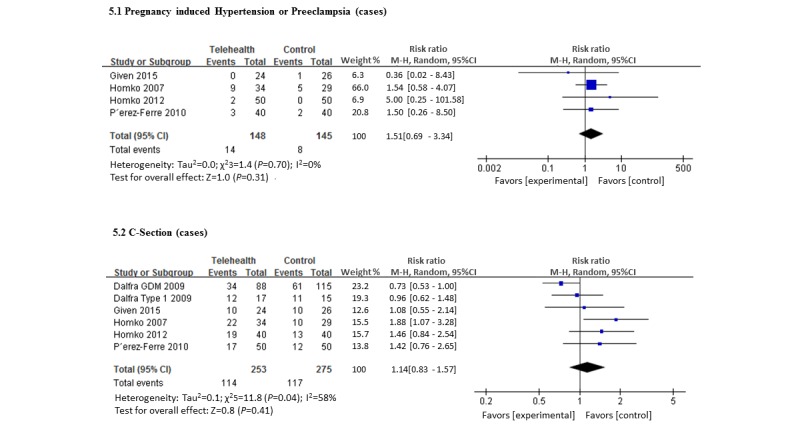
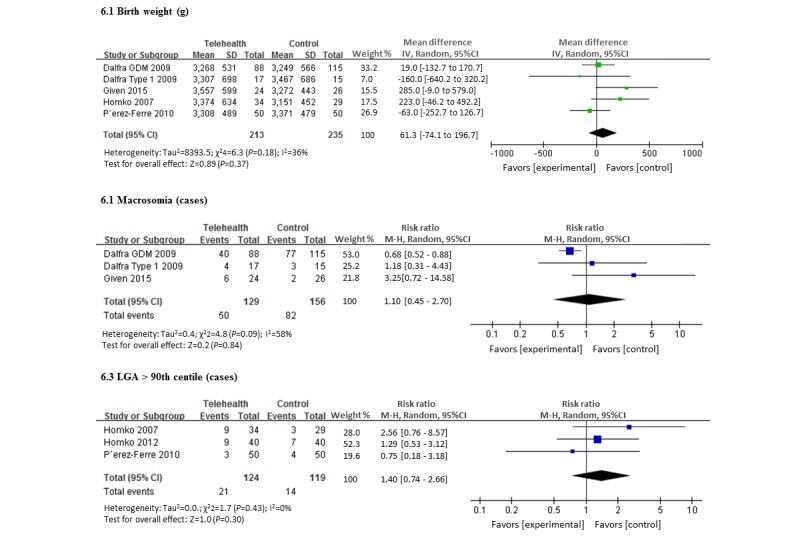
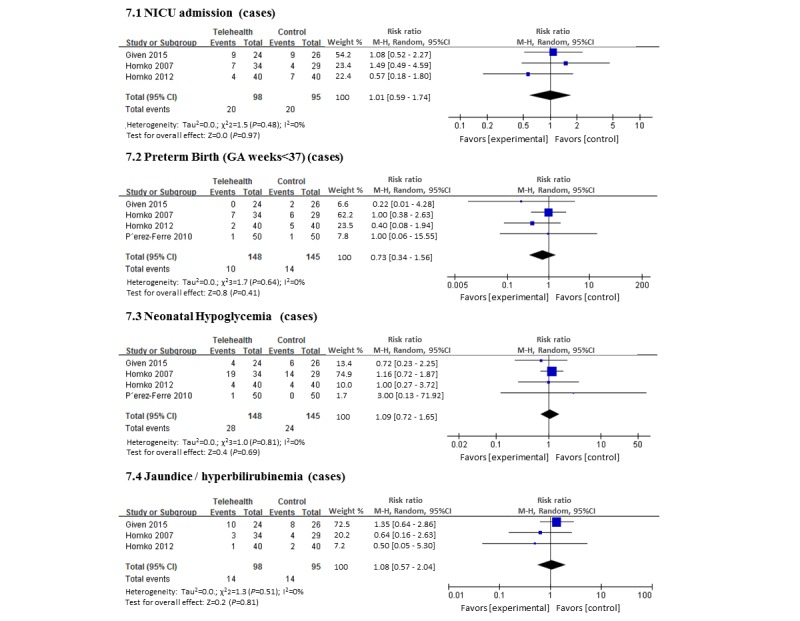
Results: A total of 7 trials were identified. Meta-analysis demonstrated a modest but statistically significant improvement in HbA1c associated with the use of a telemedicine technology. The mean HbA1c of women using telemedicine was 5.33% (SD 0.70) compared with 5.45% (SD 0.58) in the standard care group, representing a mean difference of -0.12% (95% CI -0.23% to -0.02%). When this comparison was limited to women with gestational diabetes mellitus (GDM) only, the mean HbA1c of women using telemedicine was 5.22% (SD 0.70) compared with 5.37% (SD 0.61) in the standard care group, mean difference -0.14% (95% CI -0.25% to -0.04%). There were no differences in other maternal and neonatal outcomes reported.
Conclusions: There is currently insufficient evidence that telemedicine technology is superior to standard care for women with diabetes in pregnancy; however, there was no evidence of harm. No trials were identified that assessed patient satisfaction or cost of care delivery, and it may be in these areas where these technologies may be found most valuable.
Keywords: diabetes mellitus; meta-analysis; pregnancy; pregnancy in diabetics; review; telemedicine.
©Wai-Kit Ming, Lucy H Mackillop, Andrew J Farmer, Lise Loerup, Katy Bartlett, Jonathan C Levy, Lionel Tarassenko, Carmelo Velardo, Yvonne Kenworthy, Jane E Hirst. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 09.11.2016.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- IDF. [2016-10-27]. IDF Diabetes Atlas reveals high burden of hyperglycaemia in pregnancy. 2014. http://www.idf.org/diabetesvoice/issue-1-2014/idf-diabetes-atlas .
-
- Balsells M, García-Patterson A, Solà I, Roqué M, Gich I, Corcoy R. Glibenclamide, metformin, and insulin for the treatment of gestational diabetes: a systematic review and meta-analysis. BMJ. 2015;350:h 102. http://www.bmj.com/cgi/pmidlookup?view=long&pmid=25609400 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
