

RBC Distribution Width: Biomarker for Red Cell Dysfunction and Critical Illness Outcome?
- PMID: 27832023
- PMCID: PMC5291765
- DOI: 10.1097/PCC.0000000000001017
RBC Distribution Width: Biomarker for Red Cell Dysfunction and Critical Illness Outcome?
Abstract
Objectives: RBC distribution width is reported to be an independent predictor of outcome in adults with a variety of conditions. We sought to determine if RBC distribution width is associated with morbidity or mortality in critically ill children.
Design: Retrospective observational study.
Setting: Tertiary PICU.
Patients: All admissions to St. Louis Children's Hospital PICU between January 1, 2005, and December 31, 2012.
Interventions: We collected demographics, laboratory values, hospitalization characteristics, and outcomes. We calculated the relative change in RBC distribution width from admission RBC distribution width to the highest RBC distribution width during the first 7 days of hospitalization. Our primary outcome was ICU mortality or use of extracorporeal membrane oxygenation as a composite. Secondary outcomes were ICU- and ventilator-free days.
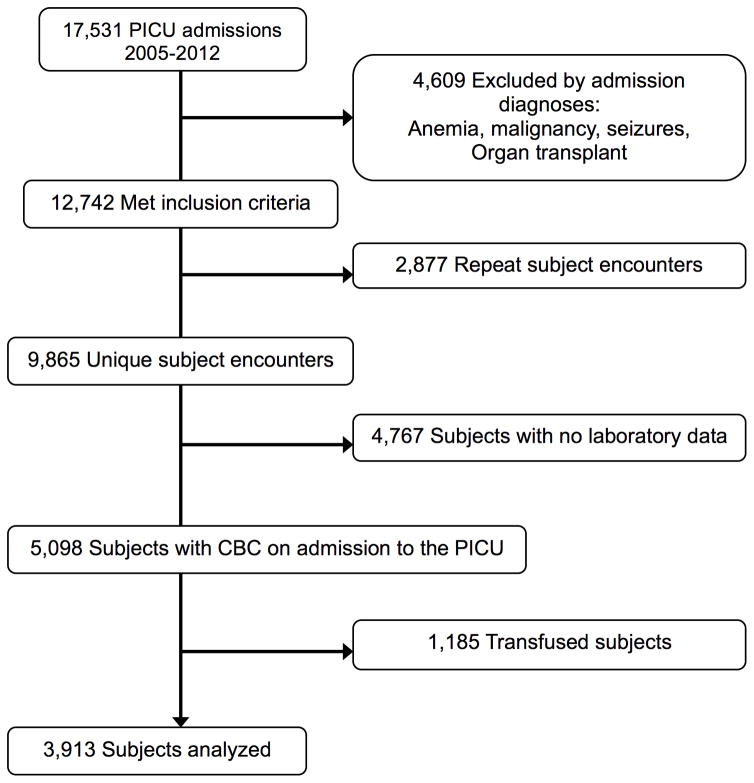
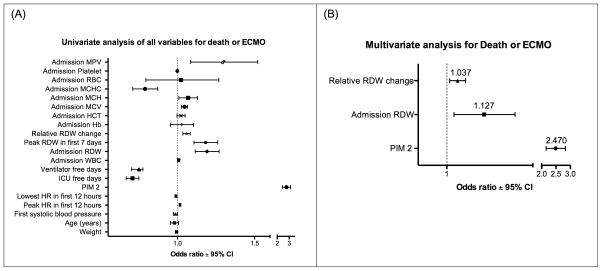
Measurements and main results: We identified 3,913 eligible subjects with an estimated mortality (by Pediatric Index of Mortality 2) of 2.94% ± 9.25% and an actual ICU mortality of 2.91%. For the study cohort, admission RBC distribution width was 14.12% ± 1.89% and relative change in RBC distribution width was 2.63% ± 6.23%. On univariate analysis, both admission RBC distribution width and relative change in RBC distribution width correlated with mortality or the use of extracorporeal membrane oxygenation (odds ratio, 1.19 [95% CI, 1.12-1.27] and odds ratio, 1.06 [95% CI, 1.04-1.08], respectively; p < 0.001). After adjusting for confounding variables, including severity of illness, both admission RBC distribution width (odds ratio, 1.13; 95% CI, 1.03-1.24) and relative change in RBC distribution width (odds ratio, 1.04; 95% CI, 1.01-1.07) remained independently associated with ICU mortality or the use of extracorporeal membrane oxygenation. Admission RBC distribution width and relative change in RBC distribution width both weakly correlated with fewer ICU- (r = 0.038) and ventilator-free days (r = 0.05) (p < 0.001).
Conclusions: Independent of illness severity in critically ill children, admission RBC distribution width is associated with ICU mortality and morbidity. These data suggest that RBC distribution width may be a biomarker for RBC injury that is of sufficient magnitude to influence critical illness outcome, possibly via oxygen delivery impairment.
Figures

Comment in
-
RBC Distribution Width: Old Dog, New Trick?Pediatr Crit Care Med. 2017 Feb;18(2):193-194. doi: 10.1097/PCC.0000000000001033. Pediatr Crit Care Med. 2017. PMID: 28157796 No abstract available.
Similar articles
-
Red Blood Cell Distribution Width as a Pragmatic Marker for Outcome in Pediatric Critical Illness.PLoS One. 2015 Jun 9;10(6):e0129258. doi: 10.1371/journal.pone.0129258. eCollection 2015. PLoS One. 2015. PMID: 26057629 Free PMC article.
-
The association of red cell distribution width at hospital discharge and out-of-hospital mortality following critical illness*.Crit Care Med. 2014 Apr;42(4):918-29. doi: 10.1097/CCM.0000000000000118. Crit Care Med. 2014. PMID: 24448196
-
Mortality of Critically Ill Children Requiring Continuous Renal Replacement Therapy: Effect of Fluid Overload, Underlying Disease, and Timing of Initiation.Pediatr Crit Care Med. 2019 Apr;20(4):314-322. doi: 10.1097/PCC.0000000000001806. Pediatr Crit Care Med. 2019. PMID: 30431556
-
Recommendations on the Indications for RBC Transfusion for the Critically Ill Child Receiving Support From Extracorporeal Membrane Oxygenation, Ventricular Assist, and Renal Replacement Therapy Devices From the Pediatric Critical Care Transfusion and Anemia Expertise Initiative.Pediatr Crit Care Med. 2018 Sep;19(9S Suppl 1):S157-S162. doi: 10.1097/PCC.0000000000001600. Pediatr Crit Care Med. 2018. PMID: 30161071 Free PMC article.
-
Association of Arterial Hyperoxia With Outcomes in Critically Ill Children: A Systematic Review and Meta-analysis.JAMA Netw Open. 2022 Jan 4;5(1):e2142105. doi: 10.1001/jamanetworkopen.2021.42105. JAMA Netw Open. 2022. PMID: 34985516 Free PMC article.
Cited by
-
Red Blood Cell Distribution Width as a Predictive Biomarker for Postoperative Infections in Children Who Underwent Cardiac Surgery: A Single-Center Retrospective Study.Cureus. 2023 Jan 22;15(1):e34051. doi: 10.7759/cureus.34051. eCollection 2023 Jan. Cureus. 2023. PMID: 36824560 Free PMC article.
-
Cross-sectional association between red blood cell distribution width and regional cerebral tissue oxygen saturation in preterm infants in the first 14 days after birth.Front Pediatr. 2023 Oct 31;11:1238762. doi: 10.3389/fped.2023.1238762. eCollection 2023. Front Pediatr. 2023. PMID: 38027304 Free PMC article.
-
Hematological Indices for Identifying Adverse Outcomes in Children Admitted to Pediatric ICUs.Cureus. 2024 Feb 6;16(2):e53744. doi: 10.7759/cureus.53744. eCollection 2024 Feb. Cureus. 2024. PMID: 38465050 Free PMC article.
-
Controlling Phlebotomy Volume Diminishes PICU Transfusion: Implementation Processes and Impact.Pediatrics. 2017 Aug;140(2):e20162480. doi: 10.1542/peds.2016-2480. Epub 2017 Jul 13. Pediatrics. 2017. PMID: 28701427 Free PMC article.
-
Altered Hemorheology in Fontan Patients in Normoxia and After Acute Hypoxic Exercise.Front Physiol. 2019 Nov 22;10:1443. doi: 10.3389/fphys.2019.01443. eCollection 2019. Front Physiol. 2019. PMID: 31824342 Free PMC article.
References
-
- Constantino B. Red cell distribution width, revisited. Laboratory Medicine. 2013;44
-
- Felker GM, Allen LA, Pocock SJ, Shaw LK, McMurray JJ, Pfeffer MA, Swedberg K, Wang D, Yusuf S, Michelson EL, Granger CB Investigators C. Red cell distribution width as a novel prognostic marker in heart failure: data from the CHARM Program and the Duke Databank. Journal of the American College of Cardiology. 2007;50:40–47. - PubMed
-
- van Kimmenade RR, Mohammed AA, Uthamalingam S, van der Meer P, Felker GM, Januzzi JL., Jr Red blood cell distribution width and 1-year mortality in acute heart failure. European Journal of Heart Failure. 2010;12:129–136. - PubMed
-
- Lee JH, Chung HJ, Kim K, Jo YH, Rhee JE, Kim YJ, Kang KW. Red cell distribution width as a prognostic marker in patients with community-acquired pneumonia. American Journal of Emergency Medicine. 2013;31:72–79. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
