

Serum Calprotectin Discriminates Subclinical Disease Activity from Ultrasound-Defined Remission in Patients with Rheumatoid Arthritis in Clinical Remission
- PMID: 27832086
- PMCID: PMC5104448
- DOI: 10.1371/journal.pone.0165498
Serum Calprotectin Discriminates Subclinical Disease Activity from Ultrasound-Defined Remission in Patients with Rheumatoid Arthritis in Clinical Remission
Abstract
Objective: Clinical remission in some patients with rheumatoid arthritis (RA) may be associated with ongoing synovial inflammation that is not always detectable on clinical examination or reflected by laboratory tests but can be visualized by musculoskeletal ultrasound. The goal of our study was to determine the levels of serum calprotectin, a major leukocyte protein, in patients with RA in clinical remission and to investigate the ability of serum calprotectin levels to distinguish patients in ultrasound-defined remission from those with residual ultrasound subclinical inflammation.
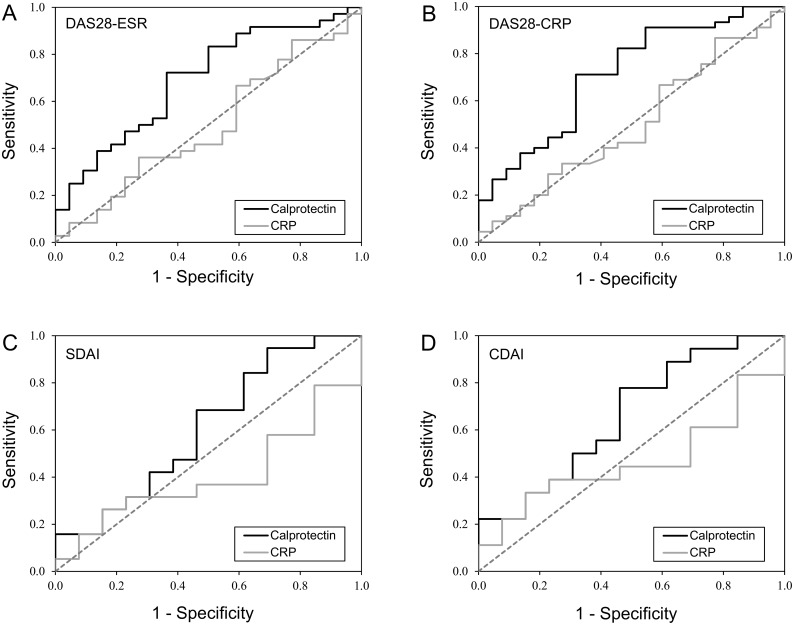
Methods: Seventy RA patients in clinical remission underwent clinical and ultrasound examination. Ultrasound examination was performed according to the German US7 score. Ultrasound remission was defined as grey scale (GS) range 0-1 and power Doppler (PD) range 0. The levels of serum calprotectin and C-reactive protein (CRP) were determined. The discriminatory capacity of calprotectin and CRP in detecting residual ultrasound inflammation was assessed using ROC curves.
Results: The total number of patients fulfilling the DAS28-ESR, DAS28-CRP, SDAI and CDAI remission criteria was 58, 67, 32 and 31, respectively. Residual synovial inflammation was found in 58-67% of the patients who fulfilled at least one set of clinical remission criteria. Calprotectin levels were significantly higher in patients with residual synovial inflammation than in those with ultrasound-defined remission (mean 2.5±1.3 vs. 1.7±0.8 μg/mL, p<0.005). Using ultrasound-defined remission criteria, calprotectin had an AUC of 0.692, p<0.05 using DAS28-ESR remission criteria and an AUC of 0.712, p<0.005 using DAS28-CRP remission criteria. Calprotectin correctly distinguished ultrasound remission from subclinical activity in 70% of patients. CRP (AUC DAS28-ESR = 0.494, p = NS; AUC DAS28-CRP = 0.498, p = NS) had lower and insignificant discriminatory capacity.
Conclusion: The present study demonstrates the potential of calprotectin to distinguish RA patients in both clinical and ultrasound-defined remission from patients in clinical remission but with residual subclinical disease activity.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


Similar articles
-
Relationship between serum calprotectin (S100A8/9) and clinical, laboratory and ultrasound parameters of disease activity in rheumatoid arthritis: A large cohort study.PLoS One. 2017 Aug 23;12(8):e0183420. doi: 10.1371/journal.pone.0183420. eCollection 2017. PLoS One. 2017. PMID: 28832684 Free PMC article.
-
Serum calprotectin (S100A8/9): an independent predictor of ultrasound synovitis in patients with rheumatoid arthritis.Arthritis Res Ther. 2015 Sep 15;17(1):252. doi: 10.1186/s13075-015-0764-5. Arthritis Res Ther. 2015. PMID: 26373925 Free PMC article.
-
Serum calprotectin may reflect inflammatory activity in patients with active rheumatoid arthritis despite normal to low C-reactive protein.Clin Rheumatol. 2018 Aug;37(8):2055-2062. doi: 10.1007/s10067-018-4091-5. Epub 2018 Apr 14. Clin Rheumatol. 2018. PMID: 29656372
-
From bench to bedside: Calprotectin (S100A8/S100A9) as a biomarker in rheumatoid arthritis.Front Immunol. 2022 Nov 3;13:1001025. doi: 10.3389/fimmu.2022.1001025. eCollection 2022. Front Immunol. 2022. PMID: 36405711 Free PMC article. Review.
-
Linkage of calprotectin with inflammation, activity and treatment response of rheumatoid arthritis: a meta-analysis.Biomark Med. 2022 Dec;16(17):1239-1249. doi: 10.2217/bmm-2022-0216. Epub 2023 Jan 20. Biomark Med. 2022. PMID: 36661047 Review.
Cited by
-
Calprotectin as a smoldering activity detection tool and renal prognosis biomarker in ANCA associated vasculitis.PLoS One. 2018 Oct 22;13(10):e0205982. doi: 10.1371/journal.pone.0205982. eCollection 2018. PLoS One. 2018. PMID: 30347000 Free PMC article.
-
Assessment of Intestinal Permeability and Inflammation Bio-Markers in Patients with Rheumatoid Arthritis.Nutrients. 2023 May 19;15(10):2386. doi: 10.3390/nu15102386. Nutrients. 2023. PMID: 37242269 Free PMC article.
-
Calprotectin (S100A8/S100A9) detects inflammatory activity in rheumatoid arthritis patients receiving tocilizumab therapy.Arthritis Res Ther. 2022 Aug 19;24(1):200. doi: 10.1186/s13075-022-02887-7. Arthritis Res Ther. 2022. PMID: 35986420 Free PMC article.
-
Relationship between serum calprotectin (S100A8/9) and clinical, laboratory and ultrasound parameters of disease activity in rheumatoid arthritis: A large cohort study.PLoS One. 2017 Aug 23;12(8):e0183420. doi: 10.1371/journal.pone.0183420. eCollection 2017. PLoS One. 2017. PMID: 28832684 Free PMC article.
-
Analytical and clinical evaluation of DiaSorin Liaison® Calprotectin fecal assay adapted for serum samples.J Clin Lab Anal. 2022 Mar;36(3):e24258. doi: 10.1002/jcla.24258. Epub 2022 Feb 5. J Clin Lab Anal. 2022. PMID: 35122317 Free PMC article.
References
-
- Klareskog L, van der Heijde D, de Jager JP, Gough A, Kalden J, Malaise M, et al. Therapeutic effect of the combination of etanercept and methotrexate compared with each treatment alone in patients with rheumatoid arthritis: double-blind randomised controlled trial. Lancet. 2004;363(9410):675–81. 10.1016/S0140-6736(04)15640-7 . - DOI - PubMed
-
- Korpela M, Laasonen L, Hannonen P, Kautiainen H, Leirisalo-Repo M, Hakala M, et al. Retardation of joint damage in patients with early rheumatoid arthritis by initial aggressive treatment with disease-modifying antirheumatic drugs: five-year experience from the FIN-RACo study. Arthritis Rheum. 2004;50(7):2072–81. 10.1002/art.20351 . - DOI - PubMed
-
- Mulherin D, Fitzgerald O, Bresnihan B. Clinical improvement and radiological deterioration in rheumatoid arthritis: evidence that the pathogenesis of synovial inflammation and articular erosion may differ. Br J Rheumatol. 1996;35(12):1263–8. . - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
