

Risk Factors for Acute Kidney Injury after Congenital Cardiac Surgery in Infants and Children: A Retrospective Observational Study
- PMID: 27832187
- PMCID: PMC5104485
- DOI: 10.1371/journal.pone.0166328
Risk Factors for Acute Kidney Injury after Congenital Cardiac Surgery in Infants and Children: A Retrospective Observational Study
Abstract
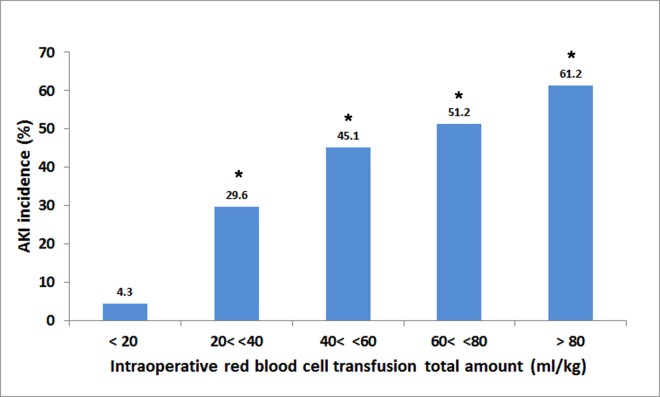
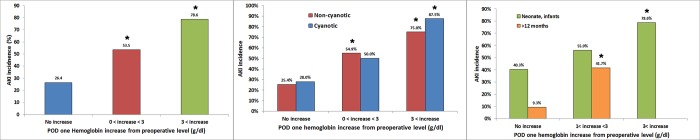
Acute kidney injury (AKI) after pediatric cardiac surgery is associated with high morbidity and mortality. Modifiable risk factors for postoperative AKI including perioperative anesthesia-related parameters were assessed. The authors conducted a single-center, retrospective cohort study of 220 patients (aged 10 days to 19 years) who underwent congenital cardiac surgery between January and December 2012. The incidence of AKI within 7 days postoperatively was determined using the Kidney Disease: Improving Global Outcomes (KDIGO) criteria. Ninety-two patients (41.8%) developed AKI and 18 (8.2%) required renal replacement therapy within the first postoperative week. Among patients who developed AKI, 57 patients (25.9%) were KDIGO stage 1, 27 patients (12.3%) were KDIGO stage 2, and eight patients (3.6%) were KDIGO stage 3. RACHS-1 (Risk-Adjusted classification for Congenital Heart Surgery) category, perioperative transfusion and fluid administration as well as fluid overload were compared between patients with and without AKI. Multivariable logistic regression analyses determined the risk factors for AKI. AKI was associated with longer hospital stay or ICU stay, and frequent sternal wound infections. Younger age (<12 months) [odds ratio (OR), 4.01; 95% confidence interval (CI), 1.77-9.06], longer cardiopulmonary bypass (CPB) time (OR, 2.45; 95% CI, 1.24-4.84), and low preoperative hemoglobin (OR, 2.40; 95% CI, 1.07-5.40) were independent risk factors for AKI. Fluid overload was not a significant predictor for AKI. When a variable of hemoglobin concentration increase (>3 g/dl) from preoperative level on POD1 was entered into the multivariable analysis, it was independently associated with postoperative AKI (OR, 6.51; 95% CI, 2.23-19.03 compared with no increase). This association was significant after adjustment with patient demographics, medication history and RACHS-1 category (hemoglobin increase >3g/dl vs. no increase: adjusted OR, 6.94; 95% CI, 2.33-20.69), regardless of different age groups and cyanotic or non-cyanotic heart disease. Prospective trials are required to evaluate whether correction of preoperative anemia and prevention of hemoconcentration may ameliorate postoperative AKI in patients who underwent congenital cardiac surgery.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
