

Radial-probe EBUS for the diagnosis of peripheral pulmonary lesions
- PMID: 27832231
- PMCID: PMC5063440
- DOI: 10.1590/S1806-37562015000000079
Radial-probe EBUS for the diagnosis of peripheral pulmonary lesions
Erratum in
-
Erratum.J Bras Pneumol. 2017 Jan-Feb;43(1):78. doi: 10.1590/S1806-37562015000000079errata. J Bras Pneumol. 2017. PMID: 28380192 Free PMC article.
Abstract
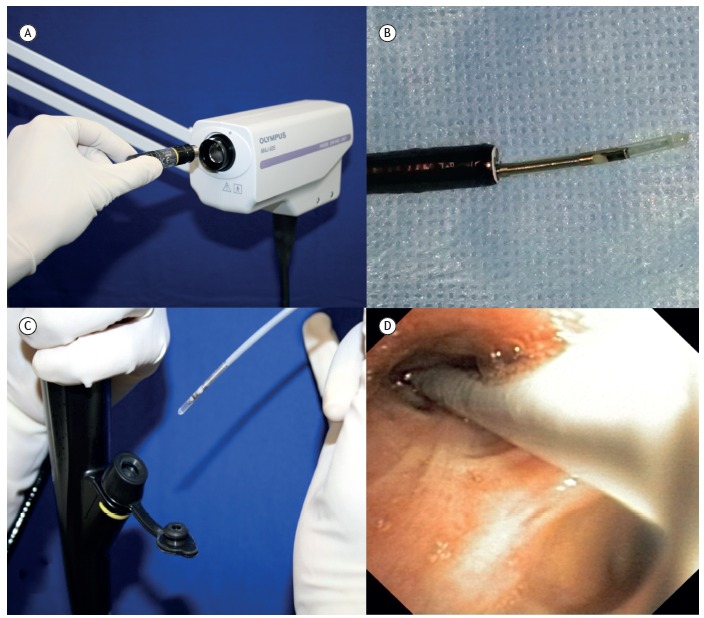
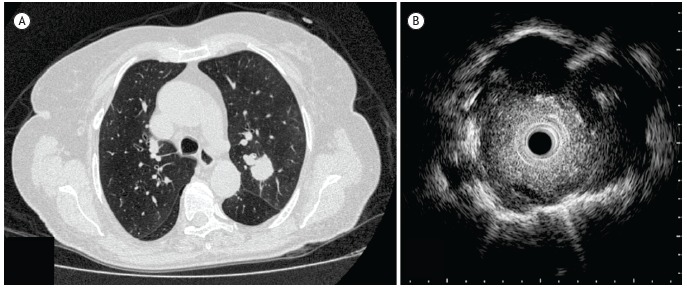
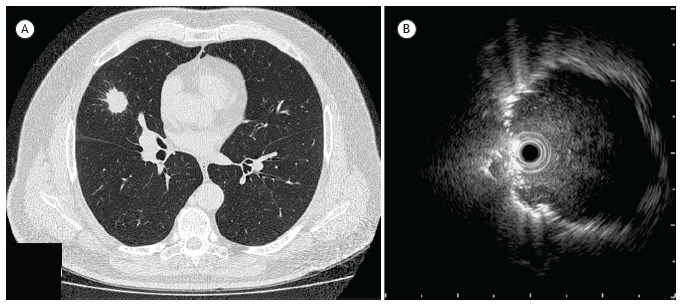
Objective:: Conventional bronchoscopy has a low diagnostic yield for peripheral pulmonary lesions. Radial-probe EBUS employs a rotating ultrasound transducer at the end of a probe that is passed through the working channel of the bronchoscope. Radial-probe EBUS facilitates the localization of peripheral pulmonary nodules, thus increasing the diagnostic yield. The objective of this study was to present our initial experience using radial-probe EBUS in the diagnosis of peripheral pulmonary lesions at a tertiary hospital.
Methods:: We conducted a retrospective analysis of 54 patients who underwent radial-probe EBUS-guided bronchoscopy for the investigation of pulmonary nodules or masses between February of 2012 and September of 2013. Radial-probe EBUS was performed with a flexible 20-MHz probe, which was passed through the working channel of the bronchoscope and advanced through the bronchus to the target lesion. For localization of the lesion and for collection procedures (bronchial brushing, transbronchial needle aspiration, and transbronchial biopsy), we used fluoroscopy.
Results:: Radial-probe EBUS identified 39 nodules (mean diameter, 1.9 ± 0.7 cm) and 19 masses (mean diameter, 4.1 ± 0.9 cm). The overall sensitivity of the method was 66.7% (79.5% and 25.0%, respectively, for lesions that were visible and not visible by radial-probe EBUS). Among the lesions that were visible by radial-probe EBUS, the sensitivity was 91.7% for masses and 74.1% for nodules. The complications were pneumothorax (in 3.7%) and bronchial bleeding, which was controlled bronchoscopically (in 9.3%).
Conclusions:: Radial-probe EBUS shows a good safety profile, a low complication rate, and high sensitivity for the diagnosis of peripheral pulmonary lesions.
Objetivo:: A broncoscopia convencional possui baixo rendimento diagnóstico para lesões pulmonares periféricas. A ecobroncoscopia radial (EBUS radial) emprega um transdutor ultrassonográfico rotatório na extremidade de uma sonda que é inserida no canal de trabalho do broncoscópio. O EBUS radial facilita a localização de nódulos pulmonares periféricos, aumentando assim o rendimento diagnóstico. O objetivo deste estudo foi apresentar nossa experiência inicial com o uso de EBUS radial para o diagnóstico de lesões pulmonares periféricas em um hospital terciário.
Métodos:: Foi realizada uma análise retrospectiva de 54 pacientes submetidos à broncoscopia guiada por EBUS radial para a investigação de nódulos ou massas pulmonares entre fevereiro de 2012 e setembro de 2013. O EBUS radial foi realizado com uma sonda flexível de 20 MHz, que foi inserida no canal de trabalho do broncoscópio até chegar à lesão-alvo. A fluoroscopia foi usada para localizar a lesão e realizar procedimentos de coleta (escovado brônquico, aspiração transbrônquica com agulha e biópsia transbrônquica).
Resultados:: O EBUS radial identificou 39 nódulos (média de diâmetro: 1,9 ± 0,7 cm) e 19 massas (média de diâmetro: 4,1 ± 0,9 cm). A sensibilidade global do EBUS radial foi de 66,7% (79,5% para as lesões visíveis pelo método e 25% para as lesões não visíveis pelo método). Nas lesões visíveis pelo método, a sensibilidade foi de 91,7% para massas e de 74,1% para nódulos. As complicações foram pneumotórax (3,7%) e sangramento brônquico controlado broncoscopicamente (9,3%).
Conclusões:: O EBUS radial apresenta bom perfil de segurança, baixo índice de complicações e alta sensibilidade para o diagnóstico de lesões pulmonares periféricas.
Objetivo:: A broncoscopia convencional possui baixo rendimento diagnóstico para lesões pulmonares periféricas. A ecobroncoscopia radial (EBUS radial) emprega um transdutor ultrassonográfico rotatório na extremidade de uma sonda que é inserida no canal de trabalho do broncoscópio. O EBUS radial facilita a localização de nódulos pulmonares periféricos, aumentando assim o rendimento diagnóstico. O objetivo deste estudo foi apresentar nossa experiência inicial com o uso de EBUS radial para o diagnóstico de lesões pulmonares periféricas em um hospital terciário.
Métodos:: Foi realizada uma análise retrospectiva de 54 pacientes submetidos à broncoscopia guiada por EBUS radial para a investigação de nódulos ou massas pulmonares entre fevereiro de 2012 e setembro de 2013. O EBUS radial foi realizado com uma sonda flexível de 20 MHz, que foi inserida no canal de trabalho do broncoscópio até chegar à lesão-alvo. A fluoroscopia foi usada para localizar a lesão e realizar procedimentos de coleta (escovado brônquico, aspiração transbrônquica com agulha e biópsia transbrônquica).
Resultados:: O EBUS radial identificou 39 nódulos (média de diâmetro: 1,9 ± 0,7 cm) e 19 massas (média de diâmetro: 4,1 ± 0,9 cm). A sensibilidade global do EBUS radial foi de 66,7% (79,5% para as lesões visíveis pelo método e 25% para as lesões não visíveis pelo método). Nas lesões visíveis pelo método, a sensibilidade foi de 91,7% para massas e de 74,1% para nódulos. As complicações foram pneumotórax (3,7%) e sangramento brônquico controlado broncoscopicamente (9,3%).
Conclusões:: O EBUS radial apresenta bom perfil de segurança, baixo índice de complicações e alta sensibilidade para o diagnóstico de lesões pulmonares periféricas.
Figures
Comment in
-
Radial-probe EBUS for the diagnosis of peripheral pulmonary lesionsAUTHORS' REPLYRadial-probe EBUS for the diagnosis of peripheral pulmonary lesionsFactors influencing visibility and diagnostic yield of transbronchial biopsy using endobronchial ultrasound in peripheral pulmonary lesionsRadial probe endobronchial ultrasound for the diagnosis of peripheral lung cancer: systematic review and meta-analysis.J Bras Pneumol. 2017 Jan-Feb;43(1):76-77. doi: 10.1590/S1806-37562016000000379. J Bras Pneumol. 2017. PMID: 28380191 Free PMC article. No abstract available.
References
-
- Rivera MP, Mehta AC. American College of Chest Physicians Initial diagnosis of lung cancer ACCP evidence-based clinical practice guidelines (2nd edition) Chest. 2007;132(3 Suppl):131S–148S. - PubMed
-
- Rivera MP, Mehta AC, Wahidi MM. Establishing the diagnosis of lung cancer Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5 Suppl):142S–165S. - PubMed
-
- Wahidi MM, Govert JA, Goudar RK, Gould MK, McCrory DC. Evidence for the treatment of patients with pulmonary nodules when is it lung cancer?: ACCP evidence-based clinical practice guidelines (2nd edition) Chest. 2007;132(3 Suppl):94S–107S. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
