

Association of Risk Factors, Mortality, and Care Costs of Adults With Acute Myeloid Leukemia With Admission to the Intensive Care Unit
- PMID: 27832254
- PMCID: PMC5344736
- DOI: 10.1001/jamaoncol.2016.4858
Association of Risk Factors, Mortality, and Care Costs of Adults With Acute Myeloid Leukemia With Admission to the Intensive Care Unit
Abstract
Importance: Adults with acute myeloid leukemia (AML) commonly require support in the intensive care unit (ICU), but risk factors for admission to the ICU and adverse outcomes remain poorly defined.
Objective: To examine risk factors, mortality, length of stay, and cost associated with admission to the ICU for patients with AML.
Design, setting, and participants: This study extracted information from the University HealthSystem Consortium database on patients 18 years or older with AML who were hospitalized for any cause between January 1, 2004, and December 31, 2012. The University HealthSystem Consortium database contains demographic, clinical, and cost variables prospectively abstracted by certified coders from discharge summaries. Outcomes were analyzed using univariate and multivariable statistical techniques. Data analysis was performed from November 15, 2013, to August 15, 2016.
Main outcomes and measures: Primary outcomes were admission to the ICU and inpatient mortality among patients requiring ICU care. Secondary outcomes included length of stay in the ICU, total hospitalization length of stay, and cost.
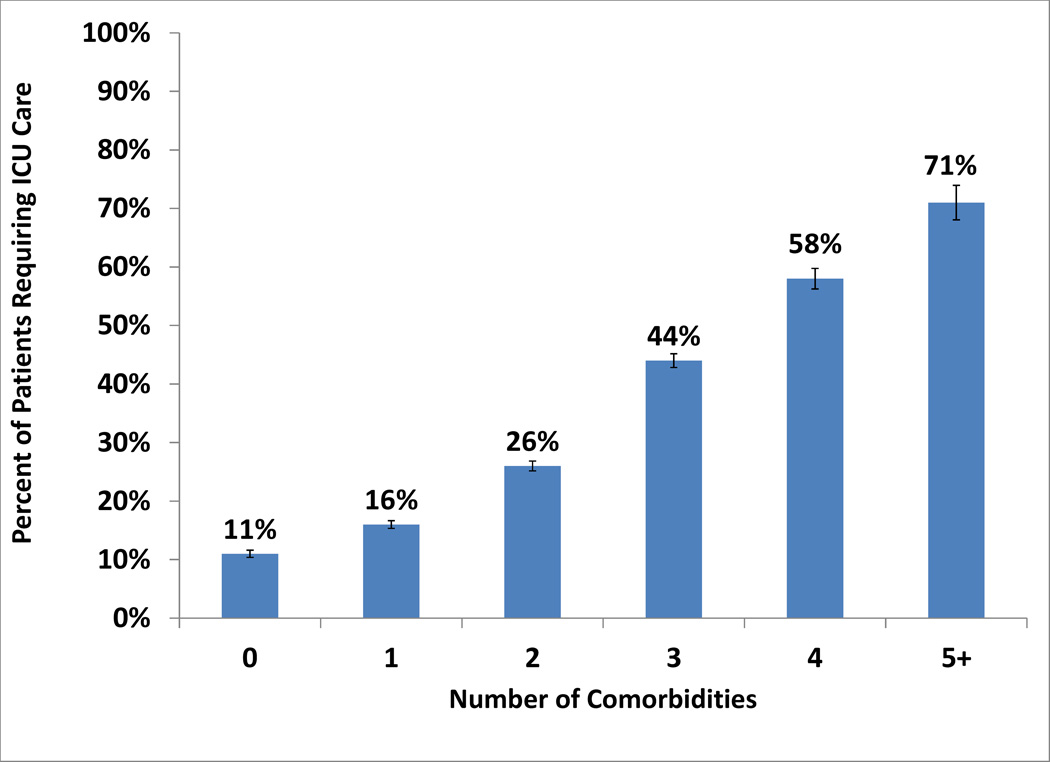
Results: Of the 43 249 patients with AML (mean [SD] age, 59.5 [16.6] years; 23 939 men and 19 310 women), 11 277 (26.1%) were admitted to the ICU. On multivariable analysis (with results reported as odds ratios [95% CIs]), independent risk factors for admission to the ICU included age younger than 80 years (1.56 [1.42-1.70]), hospitalization in the South (1.81 [1.71-1.92]), hospitalization at a low- or medium-volume hospital (1.25 [1.19-1.31]), number of comorbidities (10.64 [8.89-12.62] for 5 vs none), sepsis (4.61 [4.34-4.89]), invasive fungal infection (1.24 [1.11-1.39]), and pneumonia (1.73 [1.63-1.82]). In-hospital mortality was higher for patients requiring ICU care (4857 of 11 277 [43.1%] vs 2959 of 31 972 [9.3%]). On multivariable analysis, independent risk factors for death in patients requiring ICU care included age 60 years or older (1.16 [1.06-1.26]), nonwhite race/ethnicity (1.18 [1.07-1.30]), hospitalization on the West coast (1.19 [1.06-1.34]), number of comorbidities (18.76 [13.7-25.67] for 5 vs none), sepsis (2.94 [2.70-3.21]), invasive fungal infection (1.20 [1.02-1.42]), and pneumonia (1.13 [1.04-1.24]). Mean costs of hospitalization were higher for patients requiring ICU care ($83 354 vs $41 973) and increased with each comorbidity, from $50 543 for patients with no comorbidities to $124 820 for those with 5 or more comorbidities.
Conclusions and relevance: Admission to the ICU is associated with high mortality and cost that increase proportionally with the comorbidity burden in adults with AML. Several demographic factors and medical characteristics identify patients at risk for admission to the ICU and mortality and provide an opportunity for testing primary prevention strategies.
Figures

References
-
- Howlader NNA, Krapcho M, Garshell J, Miller D, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA, editors. SEER Cancer Statistics Review, 1975–2012. Bethesda, MD: National Cancer Institute; 2015. [based on November 2014]. http://seer.cancer.gov/csr/1975_2012/, SEER data submission, posted to the SEER web site.
-
- Azoulay E, Alberti C, Bornstain C, et al. Improved survival in cancer patients requiring mechanical ventilatory support: impact of noninvasive mechanical ventilatory support. Crit Care Med. 2001;29:519–525. - PubMed
-
- Hilbert G, Gruson D, Vargas F, et al. Noninvasive ventilation in immunosuppressed patients with pulmonary infiltrates, fever, and acute respiratory failure. N Engl J Med. 2001;344:481–487. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
