

Semi-quantitative MRI biomarkers of knee osteoarthritis progression in the FNIH biomarkers consortium cohort - Methodologic aspects and definition of change
- PMID: 27832771
- PMCID: PMC5105263
- DOI: 10.1186/s12891-016-1310-6
Semi-quantitative MRI biomarkers of knee osteoarthritis progression in the FNIH biomarkers consortium cohort - Methodologic aspects and definition of change
Abstract
Background: To describe the scoring methodology and MRI assessments used to evaluate the cross-sectional features observed in cases and controls, to define change over time for different MRI features, and to report the extent of changes over a 24-month period in the Foundation for National Institutes of Health Osteoarthritis Biomarkers Consortium study nested within the larger Osteoarthritis Initiative (OAI) Study.
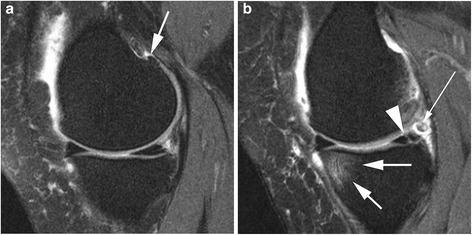
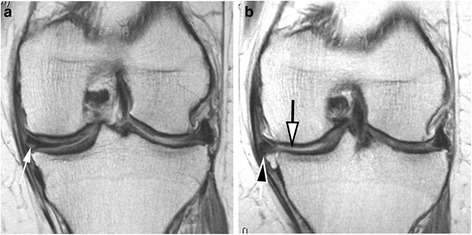
Methods: We conducted a nested case-control study. Cases (n = 406) were knees having both radiographic and pain progression. Controls (n = 194) were knee osteoarthritis subjects who did not meet the case definition. Groups were matched for Kellgren-Lawrence grade and body mass index. MRIs were acquired using 3 T MRI systems and assessed using the semi-quantitative MOAKS system. MRIs were read at baseline and 24 months for cartilage damage, bone marrow lesions (BML), osteophytes, meniscal damage and extrusion, and Hoffa- and effusion-synovitis. We provide the definition and distribution of change in these biomarkers over time.
Results: Seventy-three percent of the cases had subregions with BML worsening (vs. 66 % in controls) (p = 0.102). Little change in osteophytes was seen over 24 months. Twenty-eight percent of cases and 10 % of controls had worsening in meniscal scores in at least one subregion (p < 0.001). Seventy-three percent of cases and 53 % of controls had at least one area with worsening in cartilage surface area (p < 0.001). More cases experienced worsening in Hoffa- and effusion synovitis than controls (17 % vs. 6 % (p < 0.001); 41 % vs. 18 % (p < 0.001), respectively).
Conclusions: A wide range of MRI-detected structural pathologies was present in the FNIH cohort. More severe changes, especially for BMLs, cartilage and meniscal damage, were detected primarily among the case group suggesting that early changes in multiple structural domains are associated with radiographic worsening and symptomatic progression.
Keywords: Biomarkers; MRI; Osteoarthritis; Progression; Scoring.
Figures
Similar articles
-
Semiquantitative Imaging Biomarkers of Knee Osteoarthritis Progression: Data From the Foundation for the National Institutes of Health Osteoarthritis Biomarkers Consortium.Arthritis Rheumatol. 2016 Oct;68(10):2422-31. doi: 10.1002/art.39731. Arthritis Rheumatol. 2016. PMID: 27111771 Free PMC article.
-
Structural tissue damage and 24-month progression of semi-quantitative MRI biomarkers of knee osteoarthritis in the IMI-APPROACH cohort.BMC Musculoskelet Disord. 2022 Nov 17;23(1):988. doi: 10.1186/s12891-022-05926-1. BMC Musculoskelet Disord. 2022. PMID: 36397054 Free PMC article. Clinical Trial.
-
Evaluating the structural effects of intra-articular sprifermin on cartilage and non-cartilaginous tissue alterations, based on sqMRI assessment over 2 years.Osteoarthritis Cartilage. 2020 Sep;28(9):1229-1234. doi: 10.1016/j.joca.2020.05.015. Epub 2020 Jun 30. Osteoarthritis Cartilage. 2020. PMID: 32619609 Clinical Trial.
-
Risk factors and the natural history of accelerated knee osteoarthritis: a narrative review.BMC Musculoskelet Disord. 2020 May 29;21(1):332. doi: 10.1186/s12891-020-03367-2. BMC Musculoskelet Disord. 2020. PMID: 32471412 Free PMC article. Review.
-
MRI and non-cartilaginous structures in knee osteoarthritis.Osteoarthritis Cartilage. 2006;14 Suppl A:A87-94. doi: 10.1016/j.joca.2006.02.028. Epub 2006 May 19. Osteoarthritis Cartilage. 2006. PMID: 16713722 Review.
Cited by
-
Association between Patellofemoral and medial Tibiofemoral compartment osteoarthritis progression: exploring the effect of body weight using longitudinal data from osteoarthritis initiative (OAI).Skeletal Radiol. 2021 Sep;50(9):1845-1854. doi: 10.1007/s00256-021-03749-0. Epub 2021 Mar 8. Skeletal Radiol. 2021. PMID: 33686488
-
Biomarkers in Painful Symptomatic Knee OA Demonstrate That MRI Assessed Joint Damage and Type II Collagen Degradation Products Are Linked to Disease Progression.Front Neurosci. 2019 Oct 15;13:1016. doi: 10.3389/fnins.2019.01016. eCollection 2019. Front Neurosci. 2019. PMID: 31680799 Free PMC article.
-
Mitochondrial Genetics and Epigenetics in Osteoarthritis.Front Genet. 2020 Jan 17;10:1335. doi: 10.3389/fgene.2019.01335. eCollection 2019. Front Genet. 2020. PMID: 32010192 Free PMC article. Review.
-
Approaches to optimize analyses of multidimensional ordinal MRI data in osteoarthritis research: A perspective.Osteoarthr Cartil Open. 2024 Mar 27;6(2):100465. doi: 10.1016/j.ocarto.2024.100465. eCollection 2024 Jun. Osteoarthr Cartil Open. 2024. PMID: 38601258 Free PMC article.
-
Imaging in rheumatoid arthritis, psoriatic arthritis, axial spondyloarthritis, and osteoarthritis: An international viewpoint on the current knowledge and future research priorities.Eur J Rheumatol. 2019 Jan;6(1):38-47. doi: 10.5152/eurjrheum.2018.18121. Eur J Rheumatol. 2019. PMID: 30451654 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
