

The Psychosis Spectrum in 22q11.2 Deletion Syndrome Is Comparable to That of Nondeleted Youths
- PMID: 27832840
- PMCID: PMC5342951
- DOI: 10.1016/j.biopsych.2016.08.034
The Psychosis Spectrum in 22q11.2 Deletion Syndrome Is Comparable to That of Nondeleted Youths
Abstract
Background: Chromosome 22q11.2 deletion syndrome (22q11DS) is a promising model for studying psychosis risk. Direct comparisons of psychosis features between 22q11DS and nondeleted (ND) individuals are limited by inconsistency and small samples. In the largest study to date, we compare 22q11DS to ND in comorbidities, functioning, cognition, and psychosis features across the full range of overall severity.
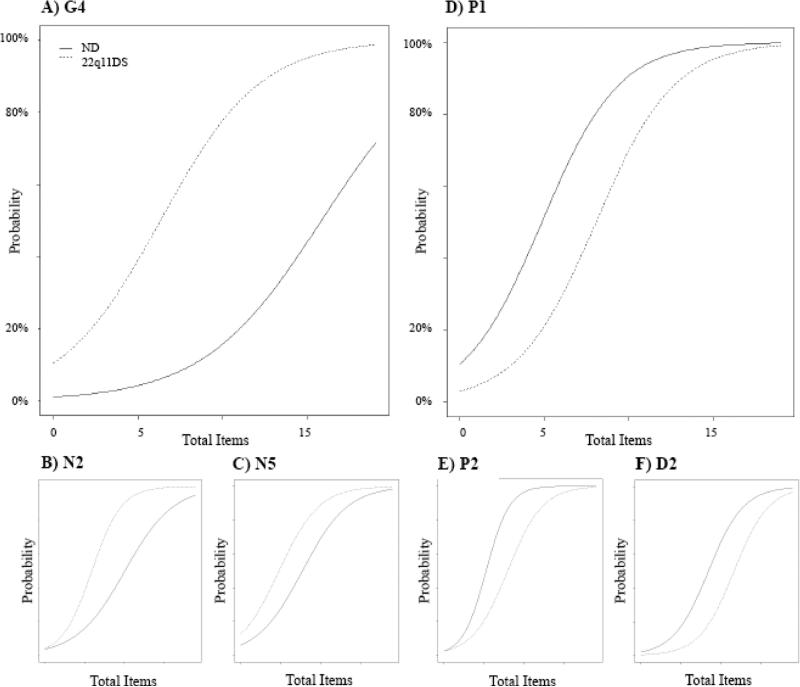
Methods: ND youths (n = 150) ages 9 to 24 years were matched to 22q11DS individuals (n = 150) on age and sex, stratifying for presence of psychosis spectrum disorder. Individuals were evaluated for psychosis using the Structured Interview for Prodromal Syndromes, and for attention-deficit/hyperactivity, substance-related, and mood disorders. Differential item functioning analysis addressed whether 22q11DS differs from ND in the probability of clinically significant ratings while holding constant the overall level of psychosis.
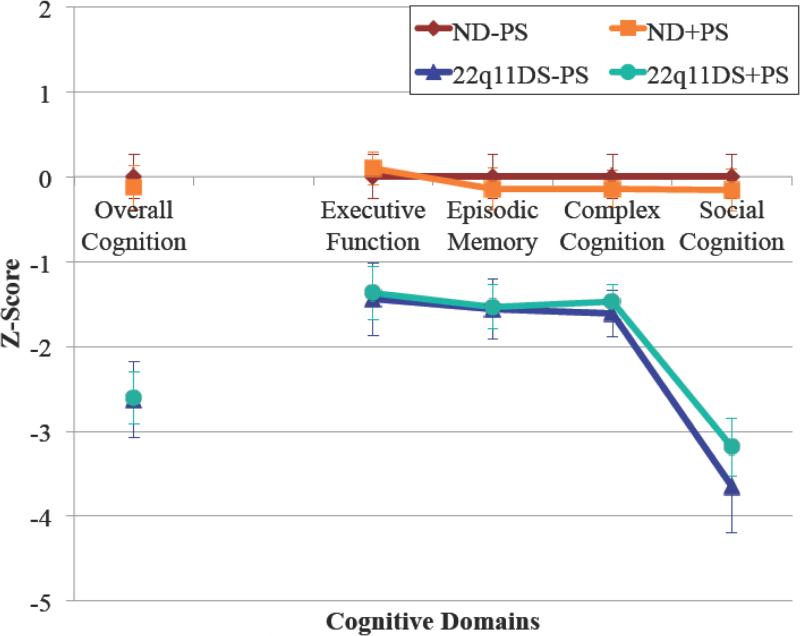
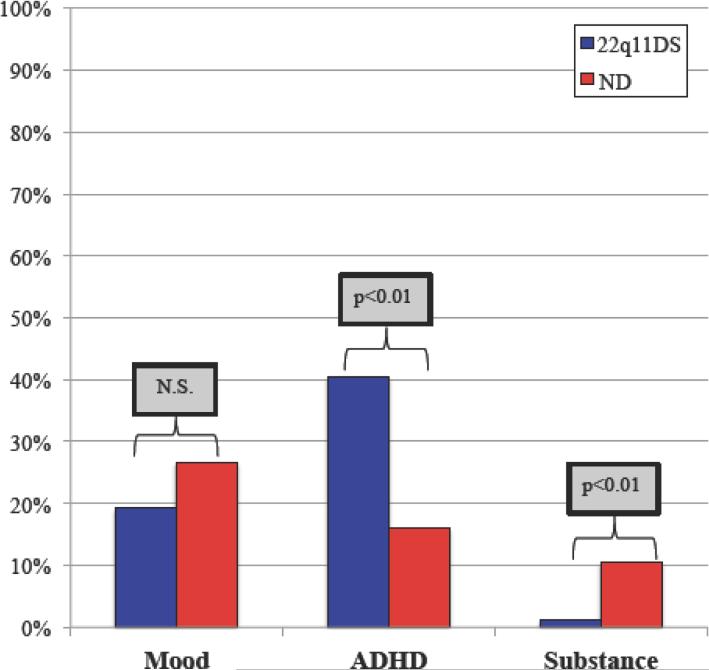
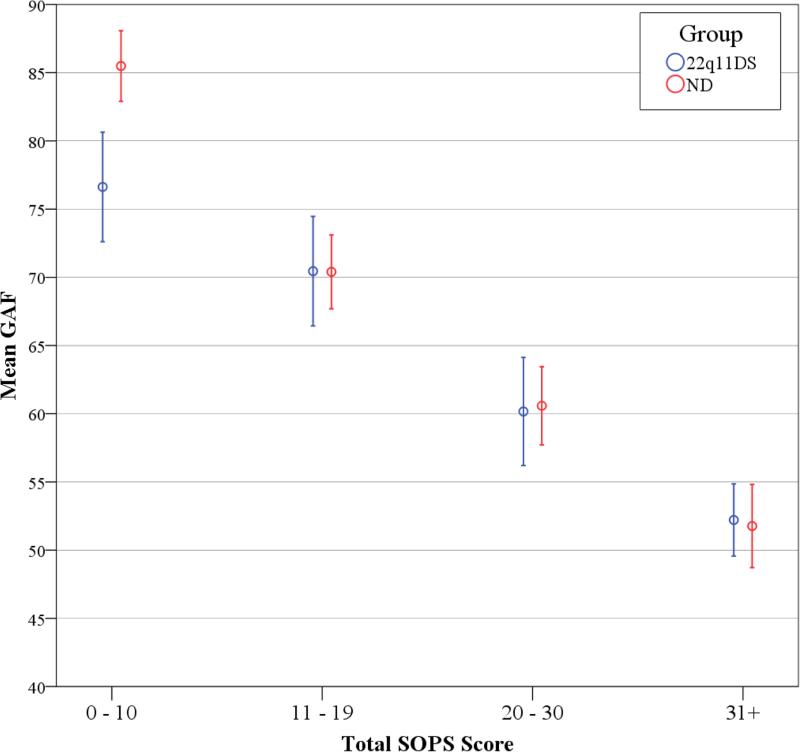
Results: Onset of psychosis proneness was similar among 22q11DS (mean: 11.0 years) and ND (mean: 12.1 years) individuals. Accounting for higher overall psychosis symptoms, 22q11DS participants were still more likely to manifest impaired stress tolerance, avolition, and ideational richness; ND individuals were more likely to exhibit unusual thoughts, persecutory ideas, and bizarre thinking. Cognition was impaired in 22q11DS, but it did not correlate with symptoms except ideational richness. Comorbid anxiety disorders were more likely in psychosis spectrum 22q11DS; substance-related disorders were more likely in ND. Global assessment of function was similar in 22q11DS and ND individuals, except among those with low total Structured Interview for Prodromal Syndromes scores.
Conclusions: Individuals with 22q11DS share overarching similarities with ND individuals in psychosis symptoms and age of onset for psychosis proneness; this continues to support the 22q11DS model as a valuable window into mechanisms contributing to psychosis.
Keywords: 22q11.2 Deletion syndrome; Clinical high risk; DiGeorge syndrome; Prodromal; Psychosis; Schizophrenia.
Copyright © 2016 Society of Biological Psychiatry. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
22q11.2 Deletion Syndrome: Characterization of Psychosis Spectrum and Future Directions.Biol Psychiatry. 2017 Jul 1;82(1):e5-e7. doi: 10.1016/j.biopsych.2017.04.002. Biol Psychiatry. 2017. PMID: 28619254 No abstract available.
Similar articles
-
Trajectories of psychiatric diagnoses and medication usage in youth with 22q11.2 deletion syndrome: a 9-year longitudinal study.Psychol Med. 2019 Aug;49(11):1914-1922. doi: 10.1017/S0033291718002696. Epub 2018 Sep 18. Psychol Med. 2019. PMID: 30226117
-
Impact of psychiatric comorbidity and cognitive deficit on function in 22q11.2 deletion syndrome.J Clin Psychiatry. 2015 Oct;76(10):e1262-70. doi: 10.4088/JCP.14m09197. J Clin Psychiatry. 2015. PMID: 26528648
-
Psychiatric disorders in 22q11.2 deletion syndrome are prevalent but undertreated.Psychol Med. 2014 Apr;44(6):1267-77. doi: 10.1017/S0033291713001669. Epub 2013 Sep 9. Psychol Med. 2014. PMID: 24016317 Free PMC article.
-
Recent developments in understanding the relationship between 22q11.2 deletion syndrome and psychosis.Curr Opin Psychiatry. 2019 Mar;32(2):67-72. doi: 10.1097/YCO.0000000000000466. Curr Opin Psychiatry. 2019. PMID: 30394904 Free PMC article. Review.
-
[Neurocognitive and psychiatric management of the 22q11.2 deletion syndrome].Encephale. 2015 Jun;41(3):266-73. doi: 10.1016/j.encep.2014.10.005. Epub 2014 Dec 16. Encephale. 2015. PMID: 25523123 Review. French.
Cited by
-
Olfactory deficits and psychosis-spectrum symptoms in 22q11.2 deletion syndrome.Schizophr Res. 2018 Dec;202:113-119. doi: 10.1016/j.schres.2018.07.012. Epub 2018 Jul 11. Schizophr Res. 2018. PMID: 30007867 Free PMC article.
-
The emergence of psychotic experiences in the early adolescence of 22q11.2 Deletion Syndrome.J Psychiatr Res. 2019 Feb;109:10-17. doi: 10.1016/j.jpsychires.2018.11.002. Epub 2018 Nov 5. J Psychiatr Res. 2019. PMID: 30458299 Free PMC article.
-
Longitudinal perspectives on the psychosis spectrum in 22q11.2 deletion syndrome.Am J Med Genet A. 2018 Oct;176(10):2192-2202. doi: 10.1002/ajmg.a.38500. Epub 2017 Oct 19. Am J Med Genet A. 2018. PMID: 29048724 Free PMC article. Review.
-
Long-term effects of early treatment with SSRIs on cognition and brain development in individuals with 22q11.2 deletion syndrome.Transl Psychiatry. 2021 May 29;11(1):336. doi: 10.1038/s41398-021-01456-x. Transl Psychiatry. 2021. PMID: 34052829 Free PMC article.
-
Psychosis Risk and Development: What Do We Know From Population-Based Studies?Biol Psychiatry. 2020 Aug 15;88(4):315-325. doi: 10.1016/j.biopsych.2019.12.014. Epub 2019 Dec 20. Biol Psychiatry. 2020. PMID: 32061373 Free PMC article. Review.
References
-
- Schneider M, Debbané M, Bassett AS, Chow EW, Fung WLA, van den Bree MB, et al. Psychiatric Disorders From Childhood to Adulthood in 22q11. 2 Deletion Syndrome: Results From the International Consortium on Brain and Behavior in 22q11. 2 Deletion Syndrome. American Journal of Psychiatry. 2014;171:627–39. - PMC - PubMed
-
- Green T, Gothelf D, Glaser B, Debbane M, Frisch A, Kotler M, et al. Psychiatric disorders and intellectual functioning throughout development in velocardiofacial (22q11.2 deletion) syndrome. J Am Acad Child Adolesc Psychiatry. 2009;48:1060–1068. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
