

Timing for Removal of Asymptomatic Long-Term Ventilation Tube in Children
- PMID: 27833863
- PMCID: PMC5083639
- DOI: 10.1007/s12070-015-0843-6
Timing for Removal of Asymptomatic Long-Term Ventilation Tube in Children
Abstract
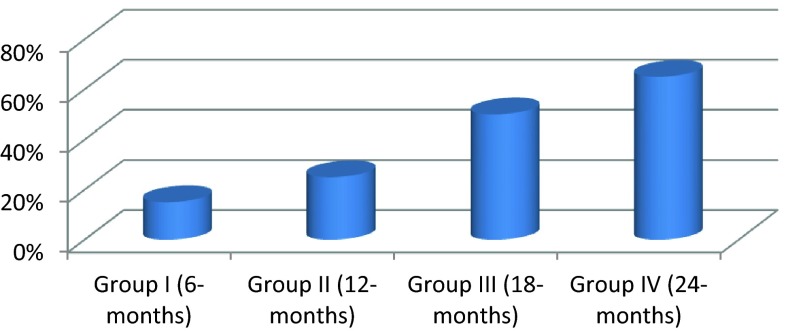
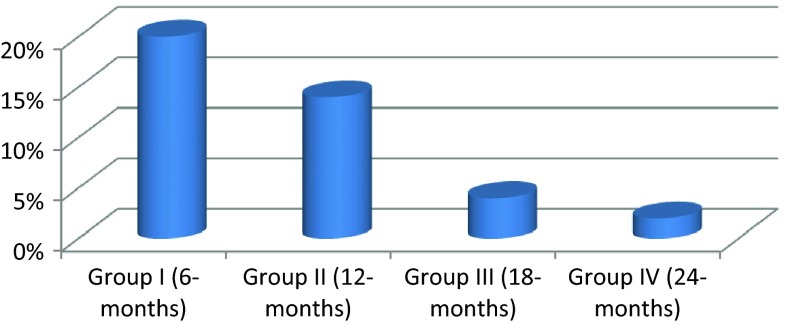
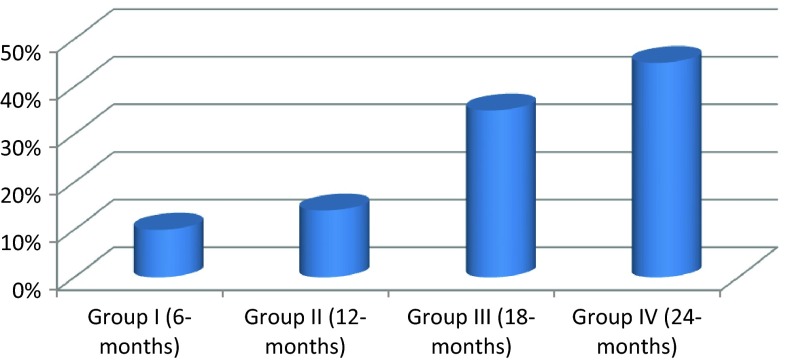
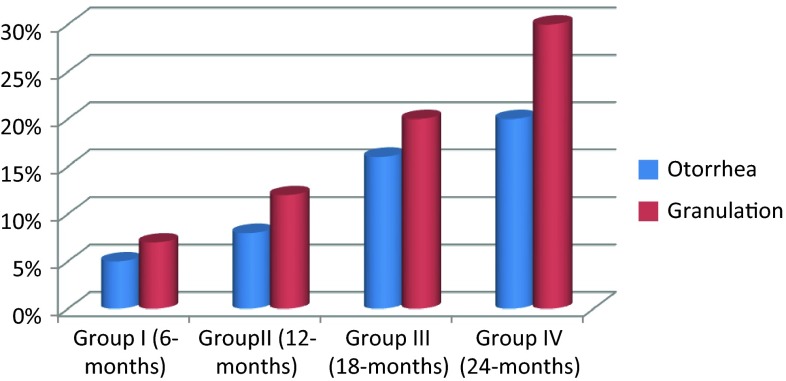
Otitis media with effusion (OME) is the most frequent illness in children. Surgical treatment options include ventilation tube insertion, adenoidectomy or both. Opinions regarding the risks, benefits and intubation period of ventilation tube insertion vary greatly. To determine the appropriate time for when to remove asymptomatic longterm ventilation T-tubes in children. In this prospective study, we analyzed the results of 120 pediatric patients (6-12 years) (240 ears) with persistent OME; we employed the Goode T-silicone tubes. We intentionally planned to remove the tubes at different time points of the study and divided our patients randomly into four subgroups with 30 patents (60 ears in each) according to the intubation period; group I: intubation for 6 months, group II: intubation for 12 months, group III: intubation for 18 months and group IV: intubation for 24 months. The relationship between intubation period and OME recurrence, the rate of persistent tympanic membrane (TM) perforation, granulation tissue or discharge near the tympanostomy tubes, normalization of Eustachian tube function and change of hearing level was analyzed in each patient group. The χ2 analysis showed that the rate of normalization of ET function was significantly higher when tubes were removed after 12-months of intubation (P = 0.002), the rate of OME recurrence was significantly higher when tubes were removed before 12-months of intubation (P = 0.004), The rate of otorrhea significantly increased after 12-months of intubation, development of granulation around tubes was significantly higher after 18-months of tube insertion. The rate of appearance of permanent TM perforation significantly increased after 18-months from tube insertion (P = 0.008). Adenoidectomy did not significantly influence the recurrence rate of OME or the rate of persistent TM peroration after tube removal. Our present results suggest that the appropriate intubation period for healing OME in children would be at 12-18 months. Also, we can conclude that longterm ventilation tubes are recommended to avoid repeated intubation and to obtain sufficient results, although their performance is not always satisfactory; mainly because of accompanying complications.
Keywords: Eustachian tube function test; Otitis media with effusion; T-Tubes; Ventilation tube.
Figures
Similar articles
-
Clinical Practice Guideline: Tympanostomy Tubes in Children (Update).Otolaryngol Head Neck Surg. 2022 Feb;166(1_suppl):S1-S55. doi: 10.1177/01945998211065662. Otolaryngol Head Neck Surg. 2022. PMID: 35138954
-
Executive Summary of Clinical Practice Guideline on Tympanostomy Tubes in Children (Update).Otolaryngol Head Neck Surg. 2022 Feb;166(2):189-206. doi: 10.1177/01945998211065661. Otolaryngol Head Neck Surg. 2022. PMID: 35138976
-
Timing for removal of tympanic ventilation tube in children.Auris Nasus Larynx. 1998 Dec;25(4):361-8. doi: 10.1016/s0385-8146(98)00022-4. Auris Nasus Larynx. 1998. PMID: 9853658
-
Otitis media with effusion.Pediatrics. 2004 May;113(5):1412-29. doi: 10.1542/peds.113.5.1412. Pediatrics. 2004. PMID: 15121966 Review.
-
Otitis media with effusion in children: Pathophysiology, diagnosis, and treatment. A review.J Otol. 2019 Jun;14(2):33-39. doi: 10.1016/j.joto.2019.01.005. Epub 2019 Jan 31. J Otol. 2019. PMID: 31223299 Free PMC article. Review.
Cited by
-
Postoperative management of pediatric tympanostomy tubes: a Yo-IFOS consensus.Eur Arch Otorhinolaryngol. 2025 Jun 27. doi: 10.1007/s00405-025-09485-8. Online ahead of print. Eur Arch Otorhinolaryngol. 2025. PMID: 40579482
-
Determination of Tympanostomy Tube Types for Otitis Media with Effusion in Patients with Cleft Palate: Comparison between Paparella Type 1 and Type 2 Tubes.J Clin Med. 2023 Oct 20;12(20):6651. doi: 10.3390/jcm12206651. J Clin Med. 2023. PMID: 37892790 Free PMC article.
-
Predictors of tympanostomy tube extrusion time in otitis media with effusion.Saudi Med J. 2022 Jul;43(7):730-734. doi: 10.15537/smj.2022.43.7.20220323. Saudi Med J. 2022. PMID: 35830986 Free PMC article.
References
-
- Kim SH, Hong HJ, Kim HJ. Effect of ventilation tube insertion on the quality of life. Korea J Otolaryngol. 2003;46:296–301.
-
- Lous J, Burton MJ, Felding J, Ovesen T, Rovers M, Williamson I. Grommets (ventilation tubes) for hearing loss associated with otitis media with effusion in children (review) Cochrane Database Syst Rev. 2010;6(10):CD00180. - PubMed
-
- Klingensmith M, Strauss M, Conner GH. A comparison of retention andcomplication rates of large-bore [Paparella II] and small-bore middle earventilating tubes. Otolaryngol Head Neck Surg. 1985;93:322–330. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources