

Progression of tau pathology within cholinergic nucleus basalis neurons in chronic traumatic encephalopathy: A chronic effects of neurotrauma consortium study
- PMID: 27834536
- PMCID: PMC5348250
- DOI: 10.1080/02699052.2016.1219058
Progression of tau pathology within cholinergic nucleus basalis neurons in chronic traumatic encephalopathy: A chronic effects of neurotrauma consortium study
Abstract
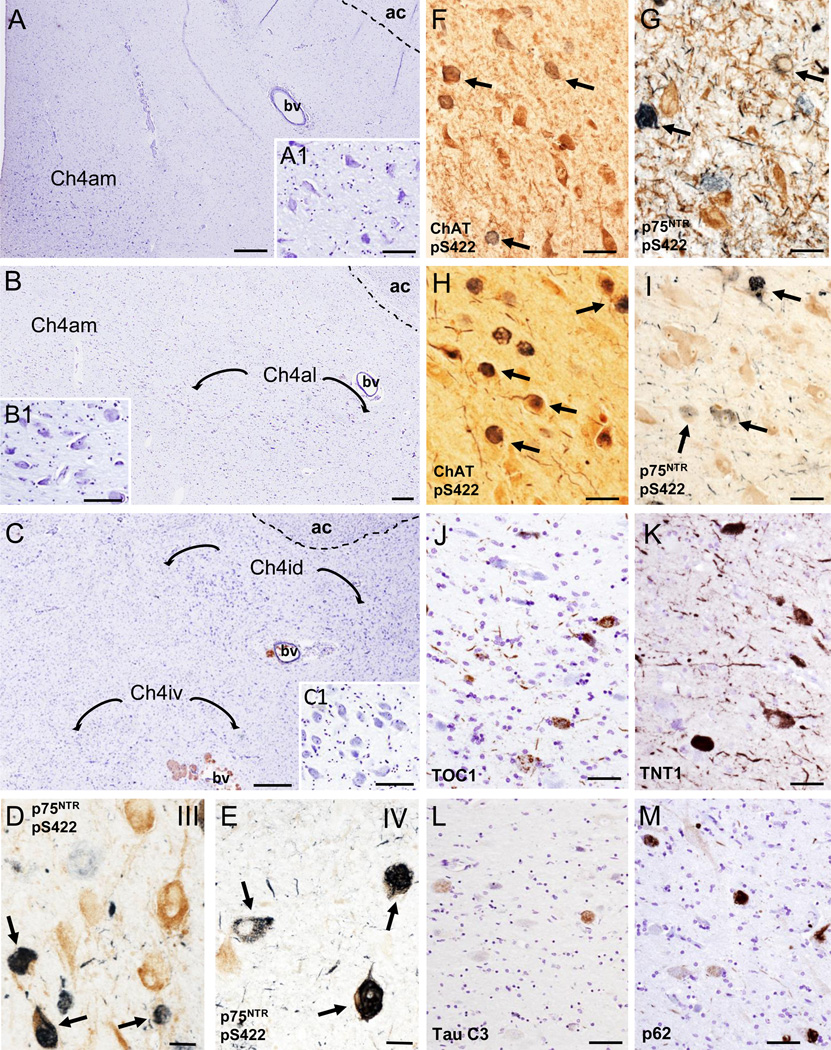
Objective: To test the hypothesis that the nucleus basalis of Meynert (nbM), a cholinergic basal forebrain (CBF) cortical projection system, develops neurofibrillary tangles (NFTs) during the progressive pathological stages of chronic traumatic encephalopathy (CTE) in the brain of athletes.
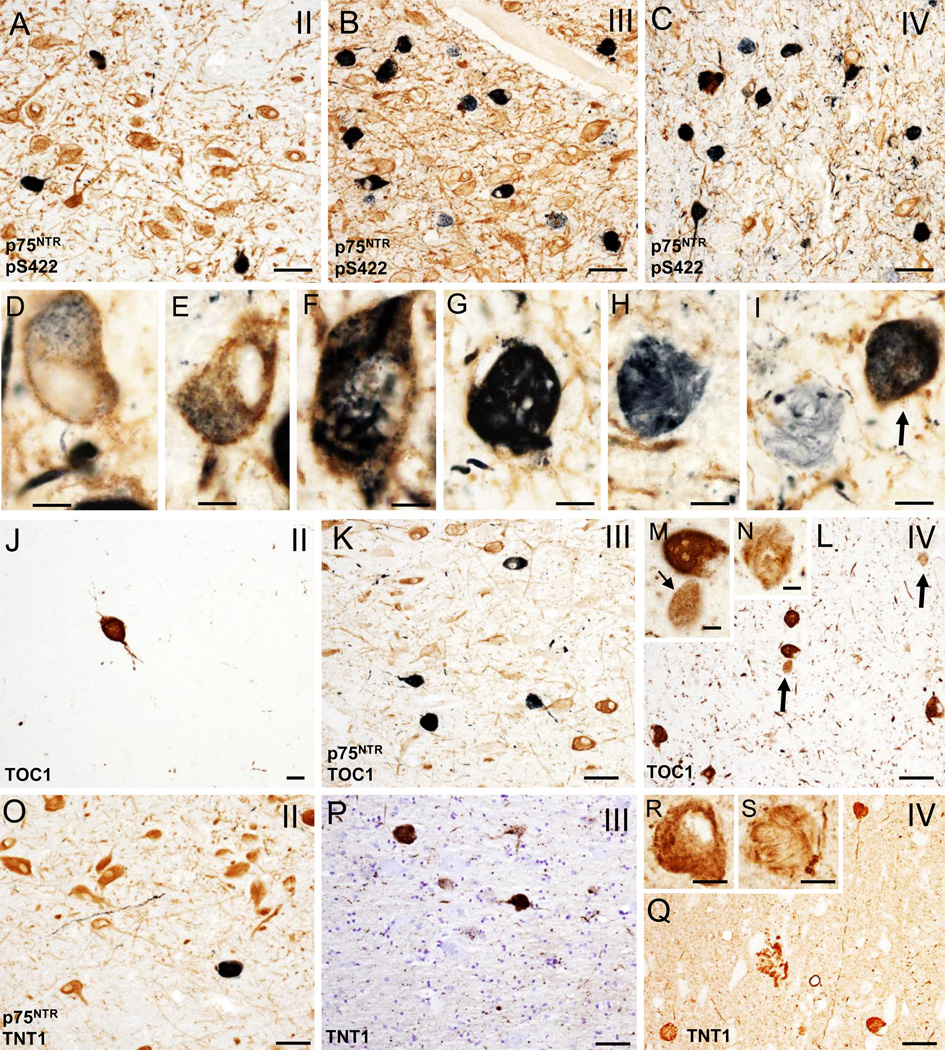
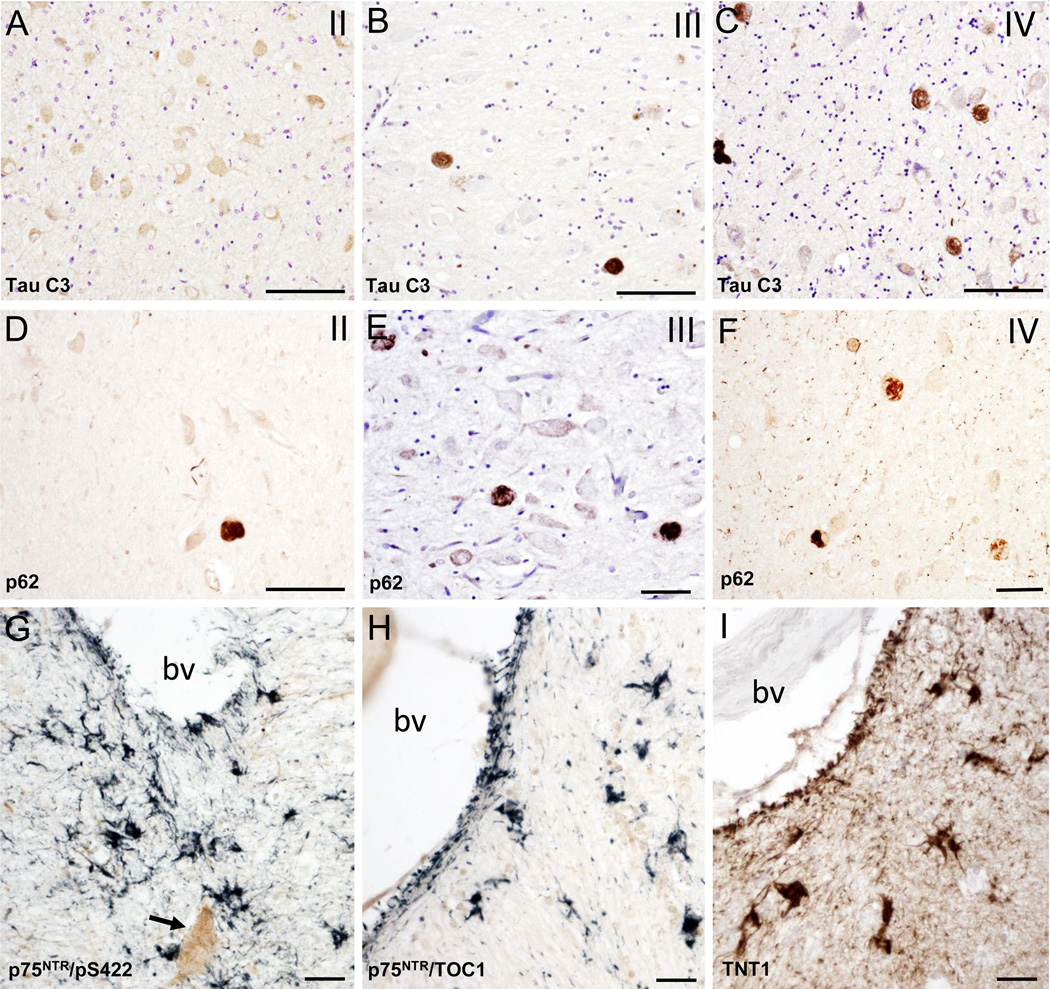
Method: To characterize NFT pathology, tau-antibodies marking early, intermediate and late stages of NFT development in CBF tissue obtained at autopsy from eighteen former athletes and veterans with a history of repetitive mild traumatic brain injury (TBI) were used.
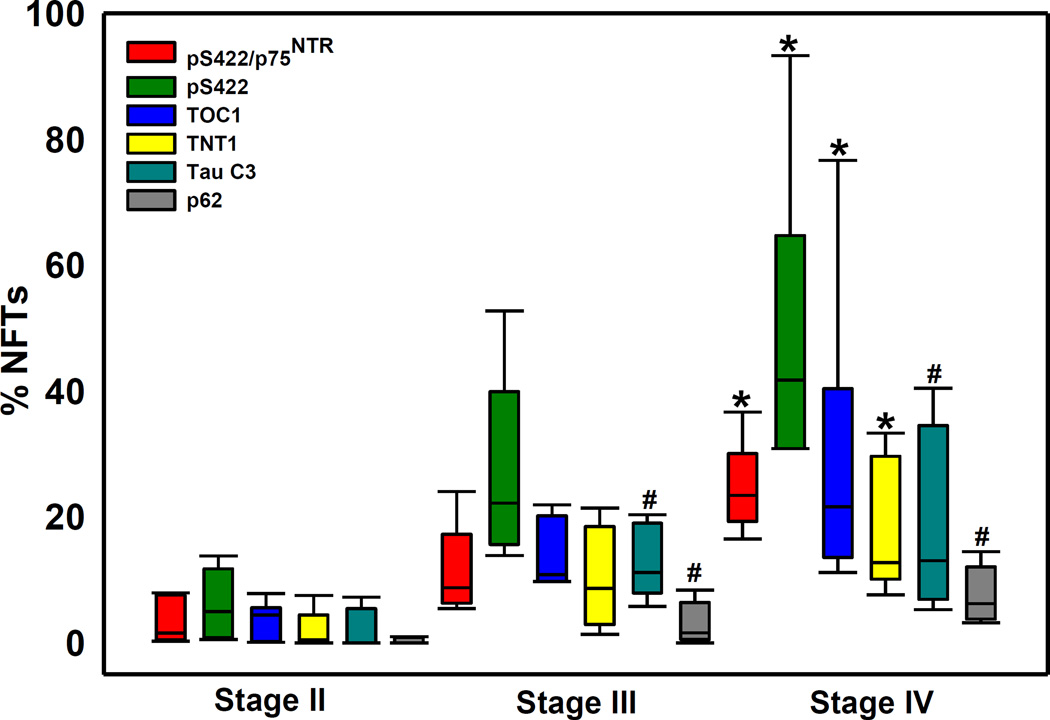
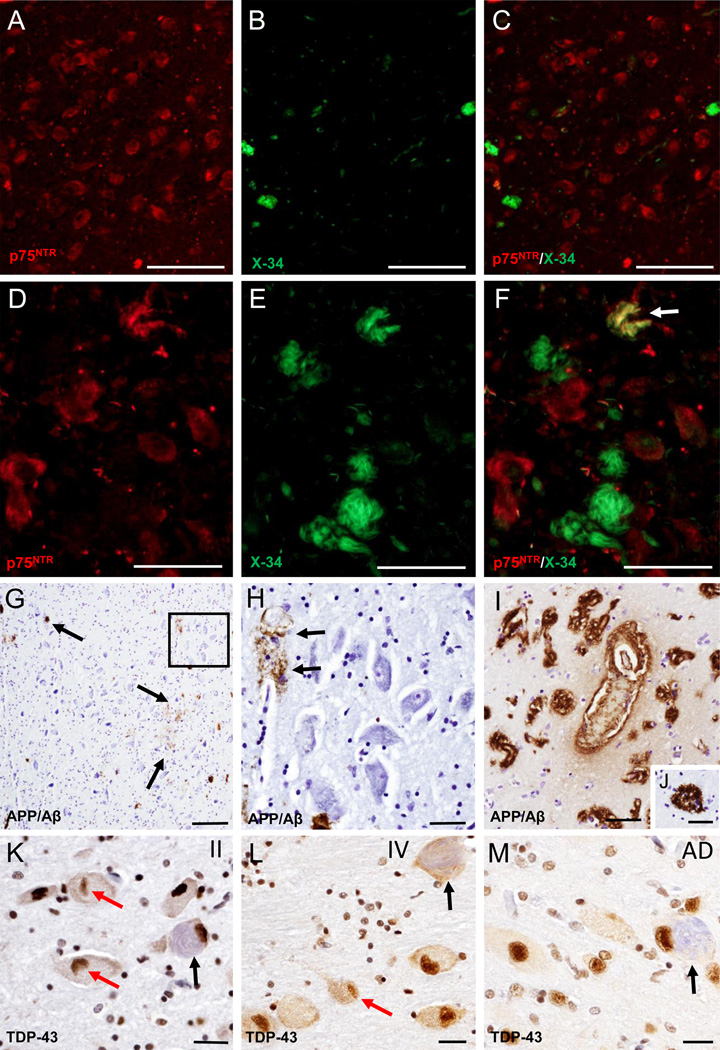
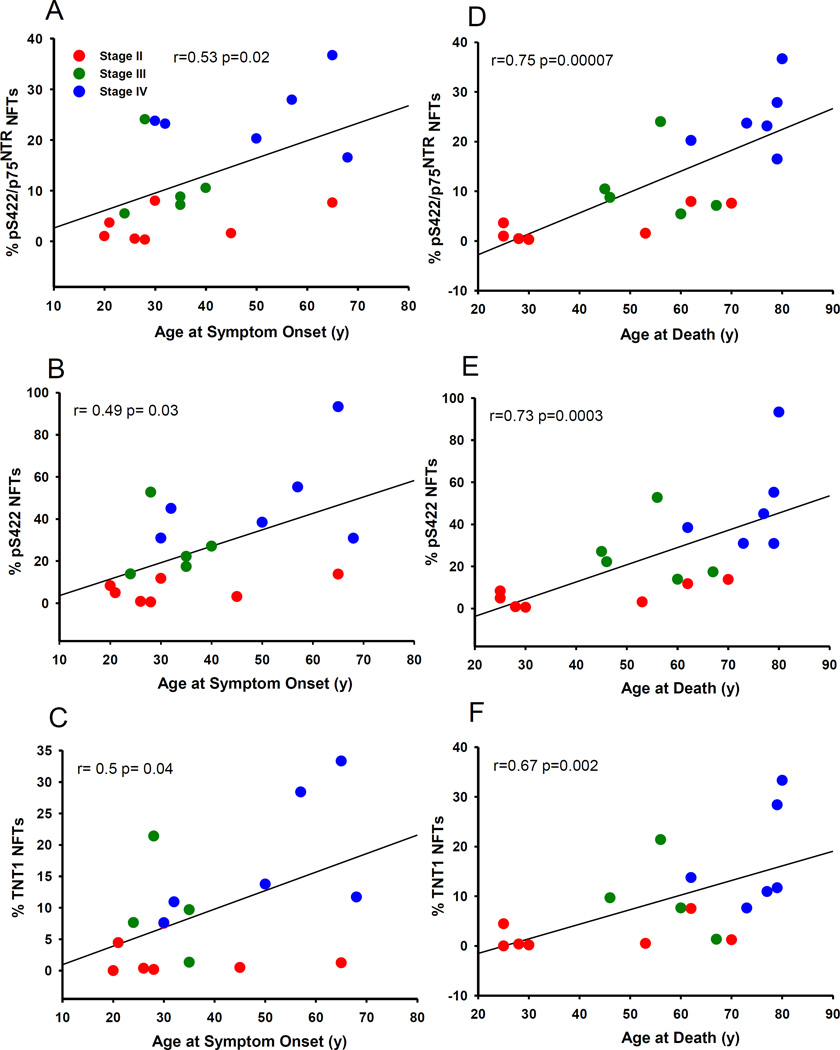
Results: Analysis revealed that cholinergic nbM neurons develop intracellular tau-immunoreactive changes progressively across the pathological stages of CTE. In particular, there was an increase in pre-tangle (phosphorylated pS422) and oligomeric (TOC1 and TNT1) forms of tau in stage IV compared to stage II CTE cases. The nbM neurons also displayed pathologic TDP-43 inclusions and diffuse extracellular and vascular amyloid-β (Aβ) deposits in CTE. A higher percentage of pS422/p75NTR, pS422 and TNT1 labelled neurons were significantly correlated with age at symptom onset, interval between symptom onset and death and age at death.
Conclusion: The development of NFTs within the cholinergic nbM neurons could contribute to an axonal disconnection in CTE. Further studies are needed to determine the mechanism driving NFT formation in the nbM neurons and its relation to chronic cognitive dysfunction in CTE.
Keywords: Cognition; head injury; memory; mild brain injury; traumatic brain injury.
Figures
References
-
- Cifu DX, Taylor BC, Carne WF, Bidelspach D, Sayer NA, Scholten J, Campbell EH. Traumatic brain injury, posttraumatic stress disorder, and pain diagnoses in OIF/OEF/OND Veterans. J Rehabil Res Dev. 2013;50:1169–1176. - PubMed
-
- Omalu B, Hammers JL, Bailes J, Hamilton RL, Kamboh MI, Webster G, Fitzsimmons RP. Chronic traumatic encephalopathy in an Iraqi war veteran with posttraumatic stress disorder who committed suicide. Neurosurg Focus. 2011;31:E3. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials