

Improved survival for patients diagnosed with chronic lymphocytic leukemia in the era of chemo-immunotherapy: a Danish population-based study of 10455 patients
- PMID: 27834937
- PMCID: PMC5148052
- DOI: 10.1038/bcj.2016.105
Improved survival for patients diagnosed with chronic lymphocytic leukemia in the era of chemo-immunotherapy: a Danish population-based study of 10455 patients
Abstract
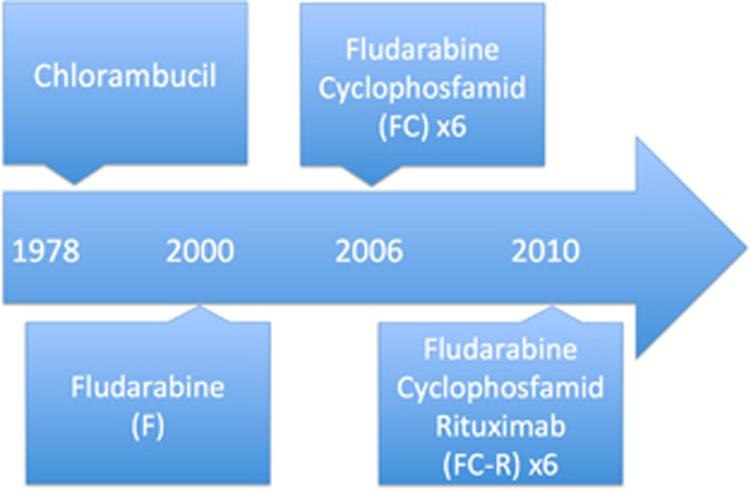
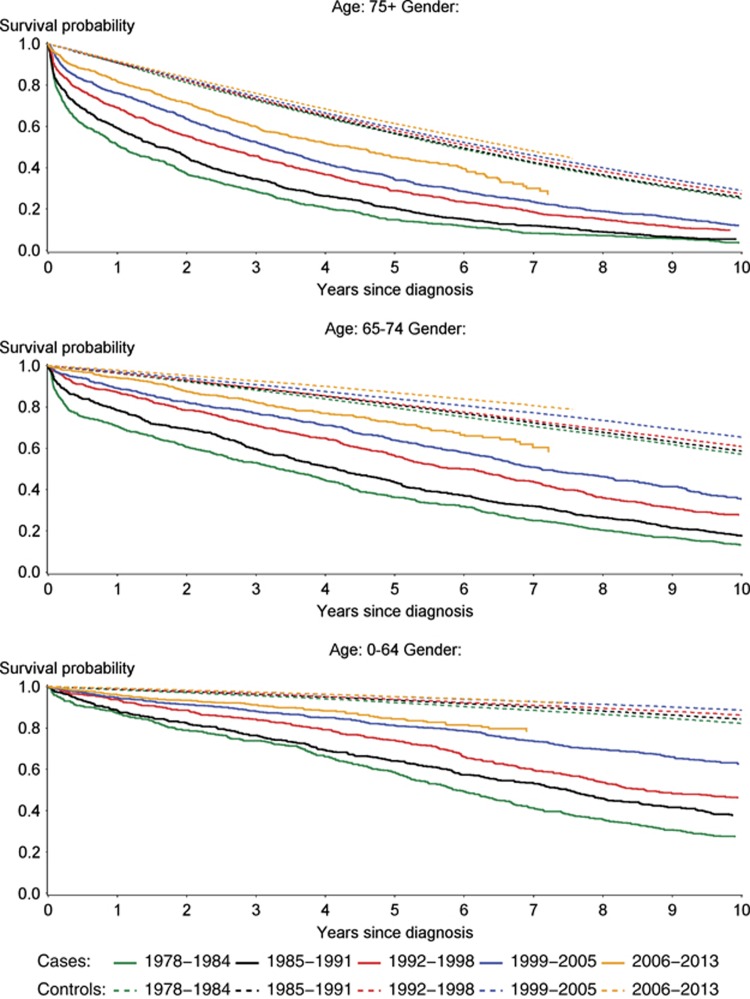
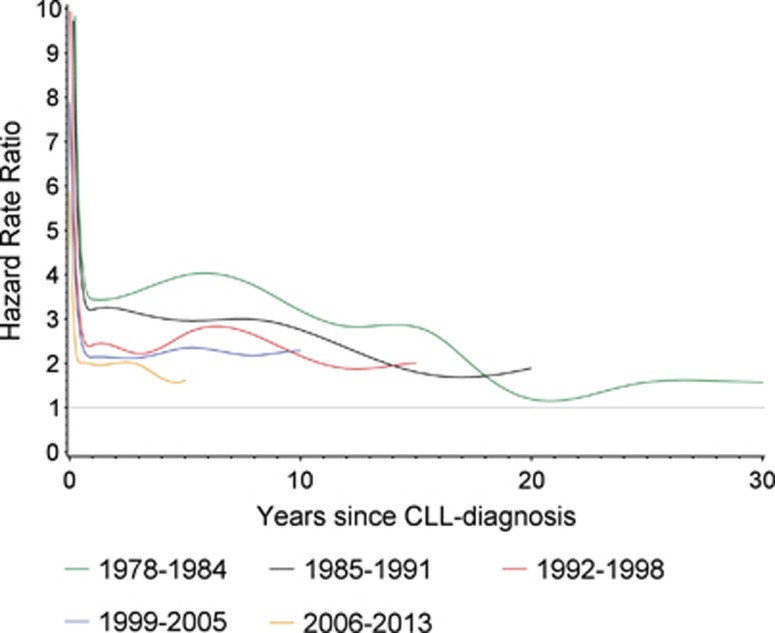
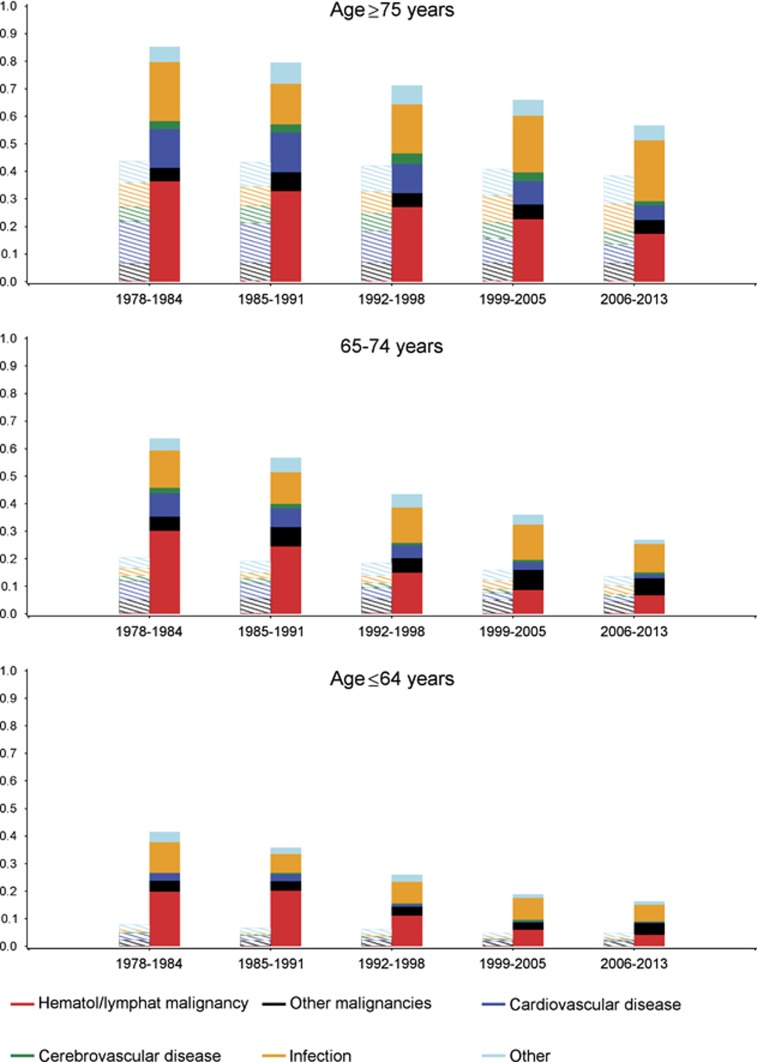
The treatment of chronic lymphocytic leukemia (CLL) is in rapid transition, and during recent decades both combination chemotherapy and immunotherapy have been introduced. To evaluate the effects of this development, we identified all CLL patients registered in the nation-wide Danish Cancer Register between 1978 and 2013. We identified 10 455 CLL patients and 508 995 CLL-free control persons from the general population. Compared with the latter, the relative mortality rate between CLL patients and their controls decreased from 3.4 (95% CI 3.2-3.6) to 1.9 (95% CI 1.7-2.1) for patients diagnosed in 1978-1984 and 2006-2013, respectively. The improved survival corresponded to a decreasing risk of death from malignant hematological diseases, whereas the risk of death from infections was stable during the study period. These population-based data substantiate the improved survival for patients treated with chemo-immunotherapy demonstrated in clinical studies.
Conflict of interest statement
CUN received consultancy fees/support outside the current study from Roche, Abbvie, Janssen, Gilead and Novartis; CG received consultancy fees from Sanofi, Celgene and Janssen and consultancy and advisory board fees from Roche outside the current study. The remaining authors declare no conflicts of interests.
Figures
References
-
- Hallek M, Cheson BD, Catovsky D, Caligaris-Cappio F, Dighiero G, Dohner H et al. Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: a report from the International Workshop on Chronic Lymphocytic Leukemia updating the National Cancer Institute-Working Group 1996 guidelines. Blood 2008; 111: 5446–5456. - PMC - PubMed
-
- Wierda WG, O'Brien S, Wang X, Faderl S, Ferrajoli A, Do KA et al. Prognostic nomogram and index for overall survival in previously untreated patients with chronic lymphocytic leukemia. Blood 2007; 109: 4679–4685. - PubMed
-
- Döhner H, Stilgenbauer S, Benner A, Leupolt E, Kröber A, Bullinger L et al. Genomic aberrations and survival in chronic lymphocytic leukemia. New Engl J Med 2000; 343: 1910–1916. - PubMed
-
- Bahlo J. The International Prognostic Index For Patients With Chronic Lymphocytic Leukaemia (CLL-IPI) - an international meta-analysis. Hematol Oncol 2015; 33: 100–180.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
