

Zika virus epidemic in Brazil. I. Fatal disease in adults: Clinical and laboratorial aspects
- PMID: 27835759
- PMCID: PMC5233712
- DOI: 10.1016/j.jcv.2016.10.024
Zika virus epidemic in Brazil. I. Fatal disease in adults: Clinical and laboratorial aspects
Abstract
Background: Zika virus (ZIKV) was first detected in Brazil in May 2015 and the country experienced an explosive epidemic. However, recent studies indicate that the introduction of ZIKV occurred in late 2013. Cases of microcephaly and deaths associated with ZIKV infection were identified in Brazil in November, 2015.
Objectives: To determine the etiology of three fatal adult cases.
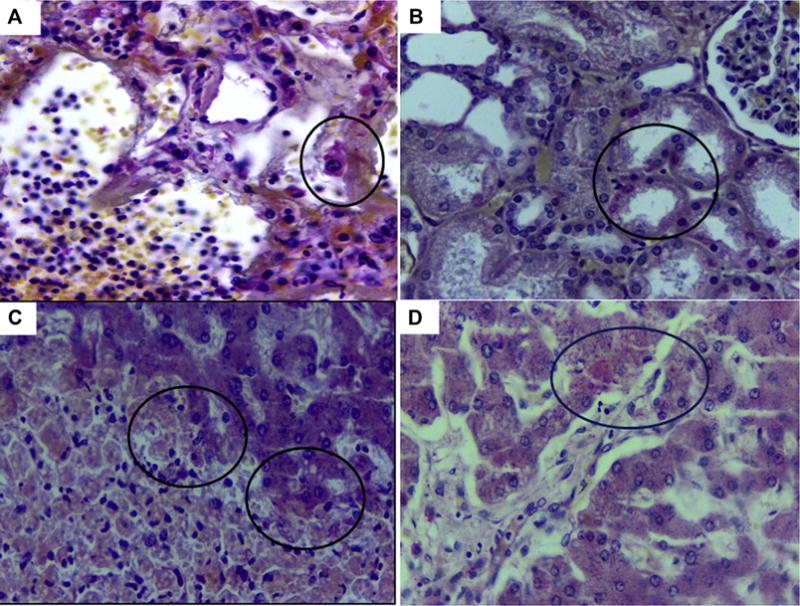
Study design: Here we report three fatal adult cases of ZIKV disease. ZIKV infection in these patients was confirmed by cells culture and/or real-time reverse transcriptase polymerase chain reaction (RT-qPCR) and by antigen detection using immunohistochemical assay. Samples of brain and other selected organs taken at autopsy from three patients were also analyzed by histopathological and immunohistological examination.
Results: The first patient, a 36-year-old man with lupus and receiving prednisone therapy, developed a fulminant ZIKV infection. At autopsy, RT-qPCR of blood and tissues was positive for ZIKV RNA, and the virus was cultured from an organ homogenate. The second patient, a previously healthy female, 16 years of age, presented classic symptoms of Zika fever, but later developed severe thrombocytopenia, anemia and hemorrhagic manifestations and died. A blood sample taken on the seventh day of her illness was positive RT-PCR for ZIKV RNA and research in the serum was positive for antinuclear factor fine speckled (1/640), suggesting Evans syndrome (hemolytic anemia an autoimmune disorder with immune thrombocytopenic purpura) secondary to ZIKV infection. The third patient was a 20-year-old woman hospitalized with fever, pneumonia and hemorrhages, who died on 13days after admission. Histopathological changes were observed in all viscera examined. ZIKV antigens were detected by immunohistochemistry in viscera specimens of patients 1 and 3. These three cases demonstrate other potential complications of ZIKV infection, in addition to microcephaly and Guillain-Barre syndrome (GBS), and they suggest that individuals with immune suppression and/or autoimmune disorders may be at higher risk of developing severe disease, if infected with ZIKV.
Keywords: Autoimmune disorders; Erythematous lupus; Evans syndrome; Histopathology; Immunohistochemistry; Zika virus.
Copyright © 2016 Elsevier B.V. All rights reserved.
Conflict of interest statement
Authors declare they have not conflict of interest.
Figures



References
-
- Dick GW. Zika virus (II). Pathogenicity and physical properties. Trans R Soc Trop Med Hyg. 1952;46:521–534. http://dx.doi.org/10.1016/0035-9203(52)90043-6. - DOI - PubMed
-
- Duffy MR, Chen TH, Hancock WT, Powers AM, Kool JL, Lanciotti RS, Pretrick M, Marfel M, Holzbauer S, Dubray C, Guillaumot L, Griggs A, Bel M, Lambert AJ, Laven J, Kosoy O, Panella A, Biggerstaff BJ, Fischer M, Hayes EB. Zika virus outbreak on yap island, federated states of Micronesia. N Engl J Med. 2009;360:2536–2543. http://dx.doi.org/10.1056/NEJMoa0805715. - DOI - PubMed
-
- Musso D, Gubler DJ. Zika virus. Clin Microbiol Rev. 2016;29:487–524. http://dx.doi.org/10.1128/CMR.00072-15. - DOI - PMC - PubMed
-
- P.A.H.O. PAHO. Zika Epidemiological Update – 29 Jul 2016. 2016 http://www.paho.org/hq/index.php?option=com_docman&task=doc_view&Itemid=....
-
- Tesh RB. A method for the isolation and identification of dengue viruses, using mosquito cell cultures. Am J Trop Med Hyg. 1979;28:1053–1059. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
