

Checkpoint Proteins in Pediatric Brain and Extracranial Solid Tumors: Opportunities for Immunotherapy
- PMID: 27836863
- PMCID: PMC5241220
- DOI: 10.1158/1078-0432.CCR-16-1829
Checkpoint Proteins in Pediatric Brain and Extracranial Solid Tumors: Opportunities for Immunotherapy
Abstract
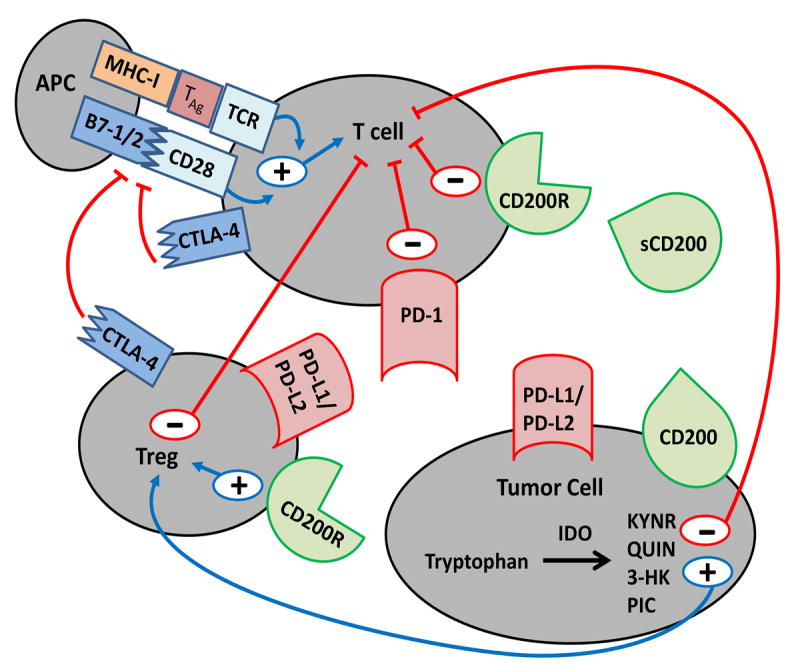
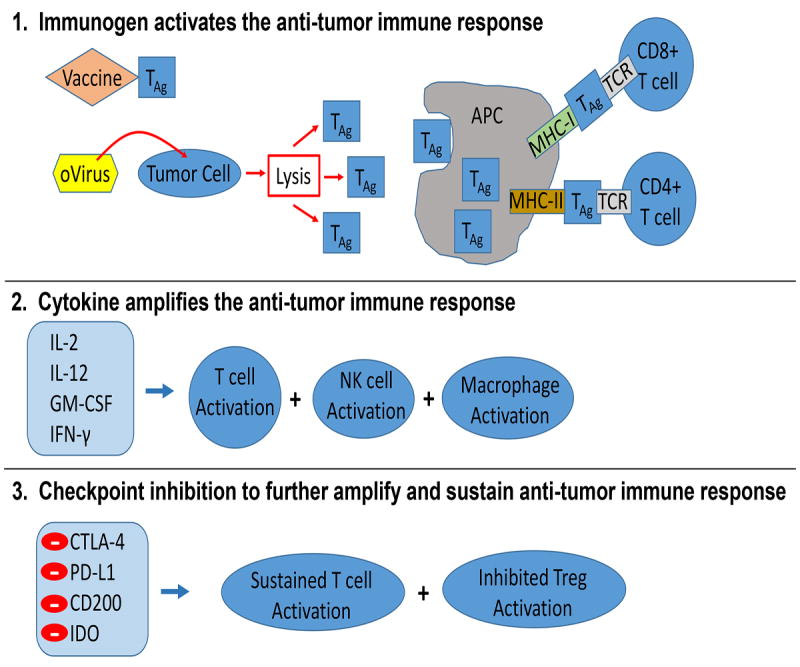
Pediatric brain and extracranial solid tumors are a diverse group of malignancies that represent almost half of all pediatric cancers. Standard therapy includes various combinations of surgery, cytotoxic chemotherapy, and radiation, which can be very harmful to a developing child, and survivors carry a substantial burden of long-term morbidities. Although these therapies have improved survival rates for children with solid tumors, outcomes still remain extremely poor for subsets of patients. Recently, immunosuppressive checkpoint molecules that negatively regulate immune cell function have been described. When found on malignant cells or in the tumor microenvironment, they contribute to immune evasion and tumor escape. Agents designed to inhibit these proteins have demonstrated significant efficacy in human adult solid tumor studies. However, there is limited research focusing on immune checkpoint molecules and inhibitors in pediatric solid tumors. In this review, we examine the current knowledge on immune checkpoint proteins with an emphasis on cytotoxic T lymphocyte antigen-4 (CTLA-4); programmed cell death protein-1 (PD-1) and programmed death-ligand 1 (PD-L1); OX-2 membrane glycoprotein (CD200); and indoleamine 2,3-dioxygenase (IDO). We review T-cell signaling, the mechanisms of action of these checkpoint molecules, pediatric preclinical studies on checkpoint proteins and checkpoint blockade, pediatric checkpoint inhibitor clinical trials conducted to date, and future immunotherapy opportunities for childhood cancers. Clin Cancer Res; 23(2); 342-50. ©2016 AACR.
©2016 American Association for Cancer Research.
Conflict of interest statement
authors have no conflicts of interest
Figures
References
-
- Ries L, Smith M, Gurney J, Linet M, Tamra T, Young J, et al. Cancer incidence and survival among children and adolescents: United States SEER Program 1975-1995. National Cancer Institute, SEER Program. NIH Pub No 99-4649; Bethesda, MD: 1999.
-
- Dong H, Strome SE, Salomao DR, Tamura H, Hirano F, Flies DB, et al. Tumor-associated B7-H1 promotes T-cell apoptosis: a potential mechanism of immune evasion. Nat Med. 2002;8:793–800. - PubMed
-
- Eggermont AM, Chiarion-Sileni V, Grob JJ, Dummer R, Wolchok JD, Schmidt H, et al. Adjuvant ipilimumab versus placebo after complete resection of high-risk stage III melanoma (EORTC 18071): a randomised, double-blind, phase 3 trial. Lancet Oncol. 2015;16:522–30. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
