

Persistence and switching patterns of oral migraine prophylactic medications among patients with chronic migraine: A retrospective claims analysis
- PMID: 27837173
- PMCID: PMC5405847
- DOI: 10.1177/0333102416678382
Persistence and switching patterns of oral migraine prophylactic medications among patients with chronic migraine: A retrospective claims analysis
Abstract
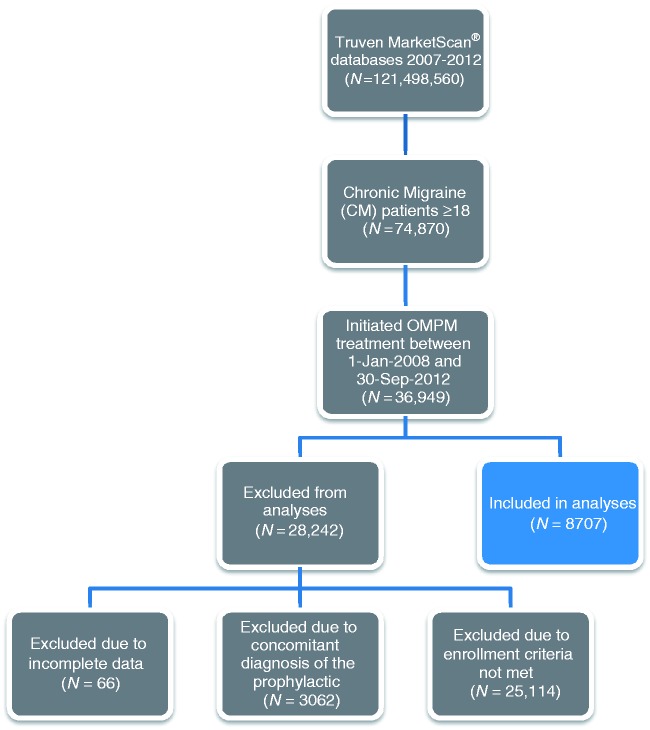
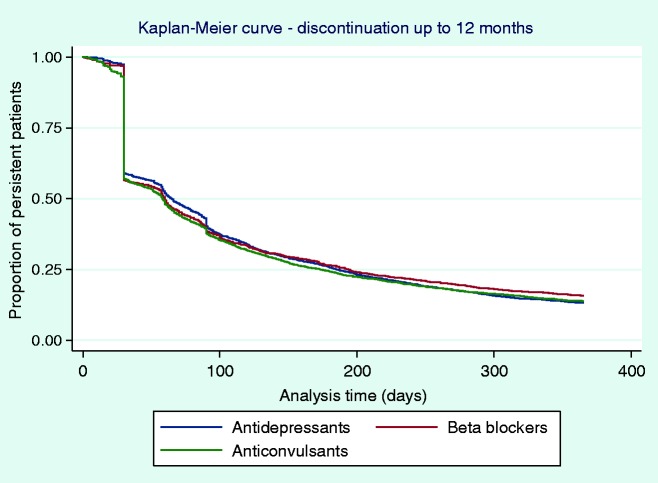
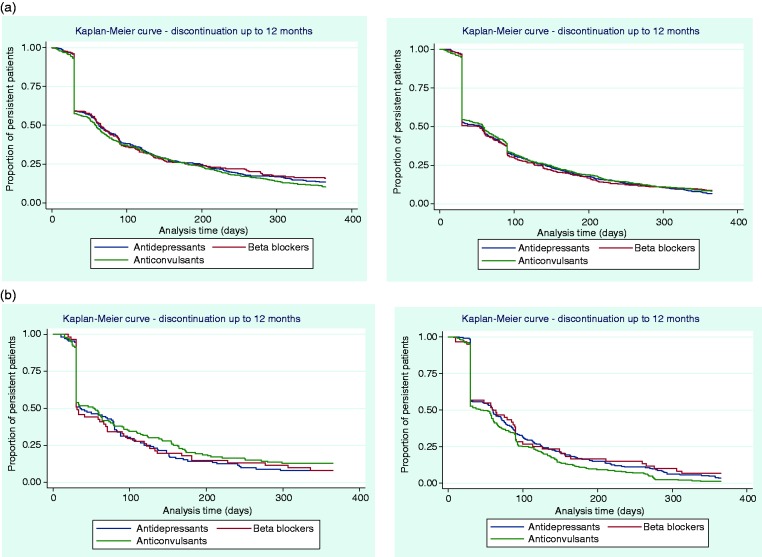
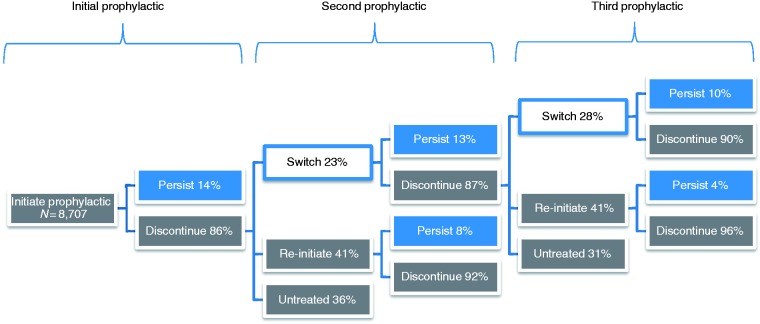
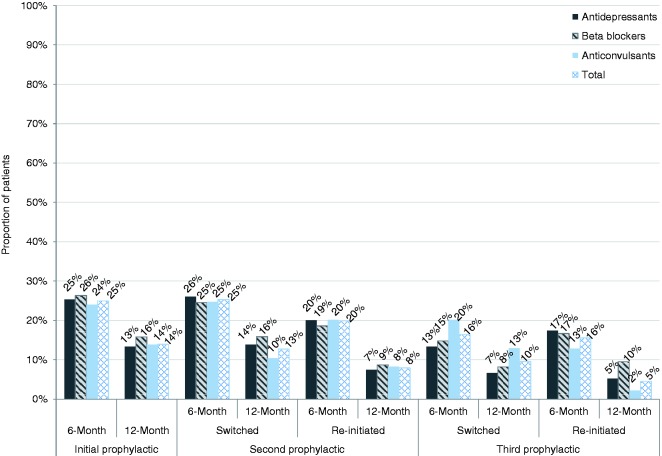
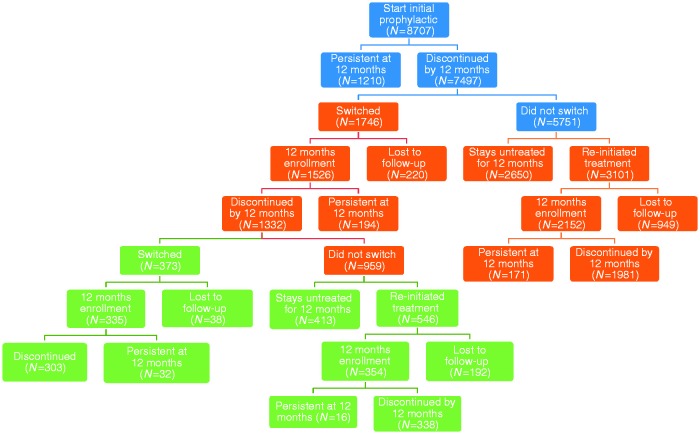
Background Migraine prevention guidelines recommend oral prophylactic medications for patients with frequent headache. This study examined oral migraine preventive medication (OMPM) treatment patterns by evaluating medication persistence, switching, and re-initiation in patients with chronic migraine (CM). Methods A retrospective US claims analysis (Truven Health MarketScan® Databases) evaluated patients ≥18 years old diagnosed with CM who had initiated an OMPM between 1 January, 2008 and 30 September, 2012. Treatment persistence was measured at six and 12 months' follow-up. Time-to-discontinuation was assessed for each OMPM and compared using Cox regression models. Among those who discontinued, the proportion that switched OMPMs within 60 days or re-initiated treatment between 61 to 365 days, and their associated persistence rates, were also assessed. Results A total of 8707 patients met the inclusion/exclusion criteria. Persistence to the initial OMPM was 25% at six months and 14% at 12 months. Based on Kaplan-Meier curves, a sharp decline of patients discontinuing was observed by 30 days, and approximately half discontinued by 60 days. Similar trends in time-to-discontinuation were seen following the second or third OMPM. Amitriptyline, gabapentin, and nortriptyline had significantly higher likelihood of non-persistence compared with topiramate. Among patients who discontinued, 23% switched to another prophylactic and 41% re-initiated therapy within one year. Among patients who switched, persistence was between 10 to 13% and among re-initiated patients, persistence was between 4 to 8% at 12 months. Conclusions Persistence to OMPMs is poor at six months and declines further by 12 months. Switching between OMPMs is common, but results indicate that persistence worsens as patients cycle through various OMPMs.
Keywords: Persistence; medication; migraine disorders/epidemiology; migraine disorders/prevention and control; patient compliance/statistics and numerical data; retrospective studies.
Figures
References
-
- Headache Classification Committee of the International Headache Society. The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013; 33: 629–808. - PubMed
-
- Buse DC, Manack AN, Fanning KM, et al. Chronic migraine prevalence, disability, and sociodemographic factors: Results from the American Migraine Prevalence and Prevention Study. Headache 2012; 52: 1456–1470. - PubMed
-
- Hazard E, Munakata J, Bigal ME, et al. The burden of migraine in the United States: Current and emerging perspectives on disease management and economic analysis. Value Health 2009; 12: 55–64. - PubMed
-
- Lipton RB, Bigal ME, Diamond M, et al. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology 2007; 68: 343–349. - PubMed
-
- Blumenfeld AM, Varon SF, Wilcox TK, et al. Disability, HRQoL and resource use among chronic and episodic migraineurs: Results from the International Burden of Migraine Study (IBMS). Cephalalgia 2011; 31: 301–315. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
