

Longitudinal Validation of the Diastolic to Systolic Time-Velocity Integral Ratio as a Doppler-Derived Measure of Pulmonary Regurgitation in Patients with Repaired Tetralogy of Fallot
- PMID: 27837302
- PMCID: PMC5332275
- DOI: 10.1007/s00246-016-1505-5
Longitudinal Validation of the Diastolic to Systolic Time-Velocity Integral Ratio as a Doppler-Derived Measure of Pulmonary Regurgitation in Patients with Repaired Tetralogy of Fallot
Abstract
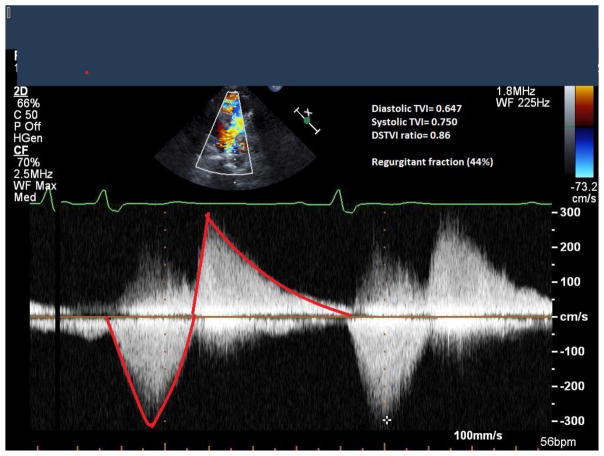
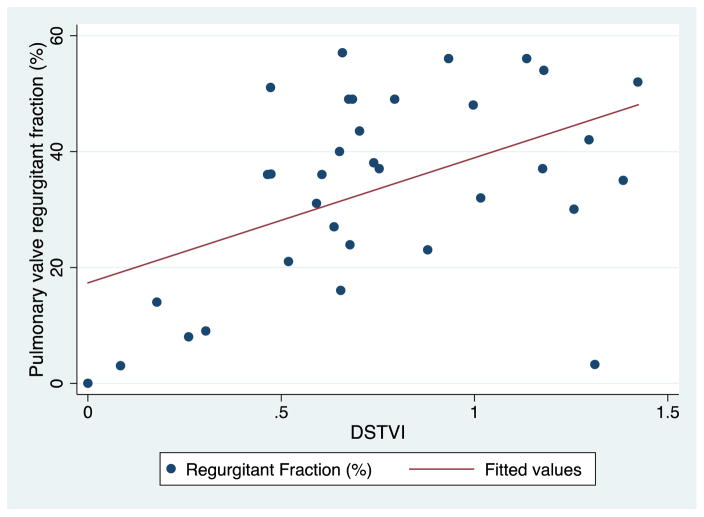
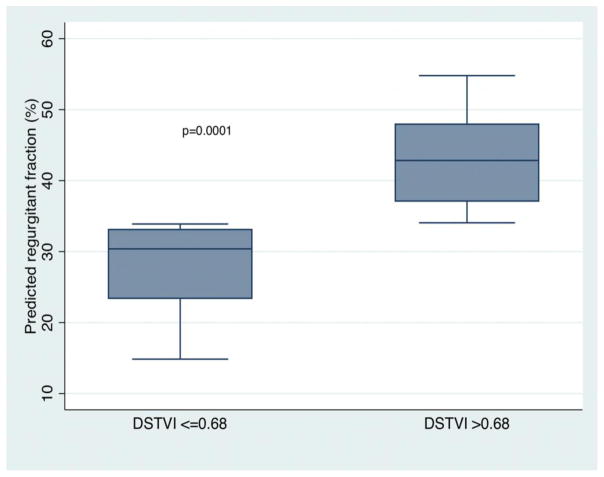
Pulmonary regurgitation (PR) is a common residual lesion and major determinant of outcome following surgical repair for tetralogy of Fallot. We sought to longitudinally study a previously described echocardiographic index as a correlate of PR measured by cardiac magnetic resonance imaging (CMR). We conducted a retrospective longitudinal study of patients with baseline and follow-up echocardiogram and CMR. The baseline studies were obtained as part of a research protocol, while the follow-up studies were performed for clinical purposes. On echocardiogram, the ratio of diastolic and systolic time-velocity integrals (DSTVI) in the main pulmonary artery was calculated. The Wilcoxon matched-pairs signed-rank test was used to test for individual changes in PR on echocardiogram and CMR. A linear regression of pulmonary valve regurgitant fraction (RF) was fit on DSTVI to identify clinically meaningful cut points of DSTVI. Thirty-five subjects were included, age at follow-up 18.3 ± 3.5 years. The follow-up between consecutive CMRs was a median time of 60 months (interquartile range 46-73). There was a moderate correlation between DSTVI and PR measured as RF by CMR (r = 0.62, p = 0.0001). A CMR RF of 20 and 40 % (the boundaries between mild/moderate and moderate/severe PR) corresponded with DSTVI of 0.52 and 0.79 (95 % CI 0.39; 0.66, and 0.69; 89), respectively. There was no significant change in either DSTVI (p = 0.61) or PR (p = 0.89) from baseline to follow-up. This study lends further credence to the DSTVI as an accurate reflection of PR. This index might become helpful in the routine echocardiographic assessment of PR. Further studies are needed to determine whether changes in RF by CMR result in changes in DSTVI.
Keywords: Echocardiogram; Pulmonary insufficiency; Regurgitation; Tetralogy of Fallot.
Figures
References
-
- Sarris GE, Comas JV, Tobota Z, Maruszewski B. Results of reparative surgery for tetralogy of Fallot: data from the European Association for Cardio-Thoracic Surgery Congenital Database. Eur J Cardiothorac Surg. 2012;42:766–74. - PubMed
-
- Alexiou C, Mahmoud H, Al-Khaddour A, et al. Outcome after repair of tetralogy of Fallot in the first year of life. Ann Thorac Surg. 2001;71:494–500. - PubMed
-
- Bacha EA, Scheule AM, Zurakowski D, et al. Long-term results after early primary repair of tetralogy of Fallot. J Thorac Cardiovasc Surg. 2001;122:154–61. - PubMed
-
- Park CS, Lee JR, Lim HG, Kim WH, Kim YJ. The long-term result of total repair for tetralogy of Fallot. Eur J Cardiothorac Surg. 2010;38:311–7. - PubMed
-
- Gatzoulis MA, Balaji S, Webber SA, et al. Risk factors for arrhythmia and sudden cardiac death late after repair of tetralogy of Fallot: a multicentre study. Lancet. 2000;356:975–81. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
