

Validation of a Risk Estimation of Tumor Recurrence After Transplant (RETREAT) Score for Hepatocellular Carcinoma Recurrence After Liver Transplant
- PMID: 27838698
- PMCID: PMC5395317
- DOI: 10.1001/jamaoncol.2016.5116
Validation of a Risk Estimation of Tumor Recurrence After Transplant (RETREAT) Score for Hepatocellular Carcinoma Recurrence After Liver Transplant
Abstract
Importance: Several factors are associated with increased hepatocellular carcinoma (HCC) recurrence after liver transplantation (LT), but no reliable risk score has been established to determine the individual risk for HCC recurrence.
Objective: We aimed to develop and validate a Risk Estimation of Tumor Recurrence After Transplant (RETREAT) score for patients with HCC meeting Milan criteria by imaging.
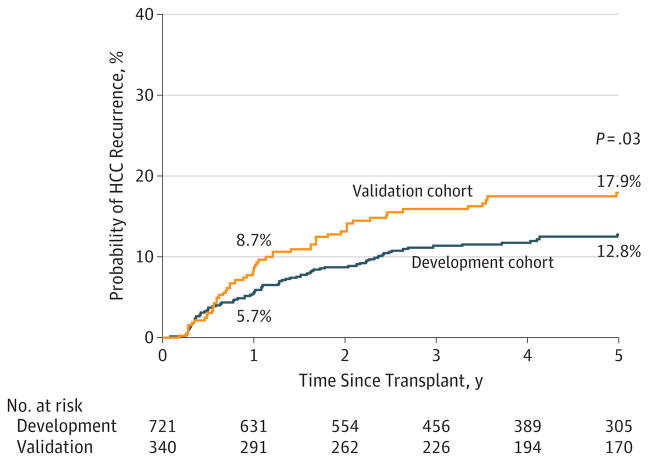
Design, setting, and participants: Predictors of recurrence were tested in a development cohort of 721 patients who underwent LT between 2002 and 2012 at 3 academic transplant centers (University of California-San Francisco; Mayo Clinic, Rochester; and Mayo Clinic, Jacksonville) to create the RETREAT score. This was subsequently validated in a cohort of 341 patients also meeting Milan criteria by imaging who underwent LT at the University of Toronto transplant center using the C concordance statistic and net reclassification index.
Main outcomes and measures: Characteristics associated with post-LT HCC recurrence.
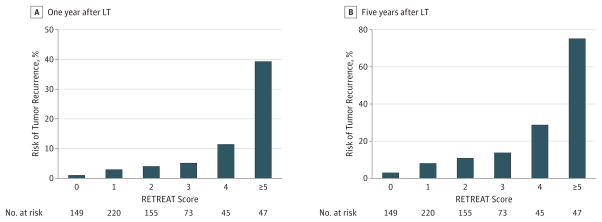
Results: A total of 1061 patients participated in the study; 77.8% (825) were men, and the median (IQR) age was 58.2 (53.3-63.9) years in the development cohort and 56.4 (51.7-61.0) years in the validation cohort (P < .001). In the development cohort of 721 patients (542 men), median α-fetoprotein (AFP) level at the time of LT was 8.3 ng/mL; 9.4% had microvascular invasion (n = 68), and 22.1% were beyond Milan criteria on explant (n = 159) owing to understaging by pretransplantation imaging. Cumulative probabilities of HCC recurrence at 1 and 5 years were 5.7% and 12.8%, respectively. On multivariable Cox proportional hazards regression, 3 variables were independently associated with HCC recurrence: microvascular invasion, AFP at time of LT, and the sum of the largest viable tumor diameter and number of viable tumors on explant. The RETREAT score was created using these 3 variables, with scores ranging from 0 to 5 or higher that were highly predictive of HCC recurrence (C statistic, 0.77). RETREAT was able to stratify 5-year post-LT recurrence risk ranging from less than 3% with a score of 0 to greater than 75% with a score of 5 or higher. The validation cohort (n = 340; 283 men) had significantly higher microvascular invasion (23.8% [n = 81], P < .001), explant beyond Milan criteria (37.3% [n = 159], P < .001), and HCC recurrence at 5 years (17.9% [n = 159], P = .03). RETREAT showed good model discrimination (C statistic, 0.82; 95% CI, 0.77-0.86) and superior recurrence risk classification compared with explant Milan criteria (net reclassification index, 0.40; P = .001) in the validation cohort.
Conclusions and relevance: We have developed and validated a simple and novel prognostic score that may improve post-LT HCC surveillance strategies and help identify patients who may benefit from future adjuvant therapies.
Conflict of interest statement
Figures
References
-
- Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334(11):693–699. - PubMed
-
- European Association for the Study of the Liver. EASL clinical practice guidelines: liver transplantation. J Hepatol. 2016;64(2):433–485. - PubMed
-
- Halazun KJ, Patzer RE, Rana AA, et al. Standing the test of time: outcomes of a decade of prioritizing patients with hepatocellular carcinoma, results of the UNOS natural geographic experiment. Hepatology. 2014;60(6):1957–1962. - PubMed
-
- Pomfret EA, Washburn K, Wald C, et al. Report of a national conference on liver allocation in patients with hepatocellular carcinoma in the United States. Liver Transpl. 2010;16(3):262–278. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
