

SDHB mutation status and tumor size but not tumor grade are important predictors of clinical outcome in pheochromocytoma and abdominal paraganglioma
- PMID: 27839933
- PMCID: PMC5164946
- DOI: 10.1016/j.surg.2016.05.050
SDHB mutation status and tumor size but not tumor grade are important predictors of clinical outcome in pheochromocytoma and abdominal paraganglioma
Abstract
Background: A staging/prognostic system has long been desired to better categorize pheochromocytoma/paraganglioma which can be very aggressive in the setting of SDHB mutations.
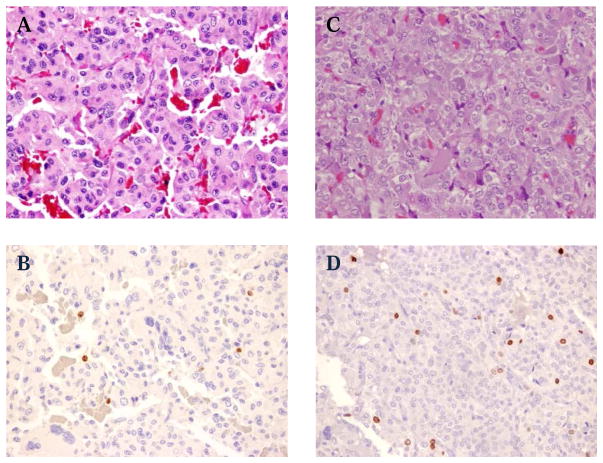
Methods: A retrospective analysis was conducted of clinical characteristics and outcomes including results of genetic testing, tumor recurrence/metastasis, Ki67/MIB1% staining, and tumor mitotic index in patients with pheochromocytoma/paraganglioma.
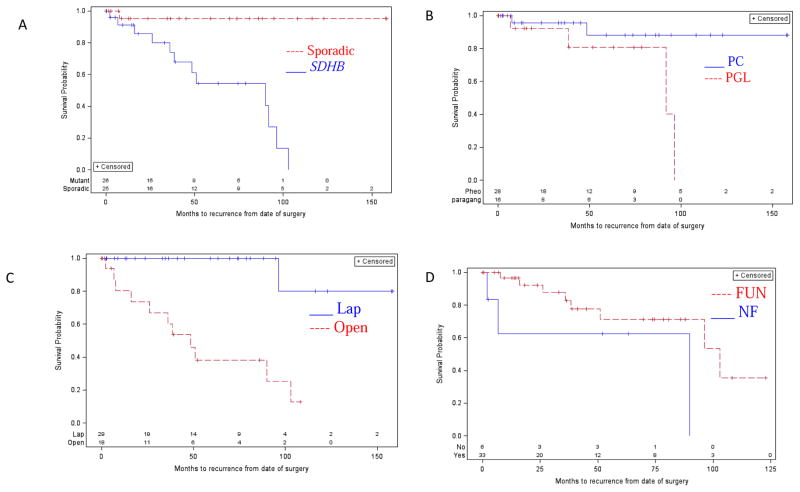
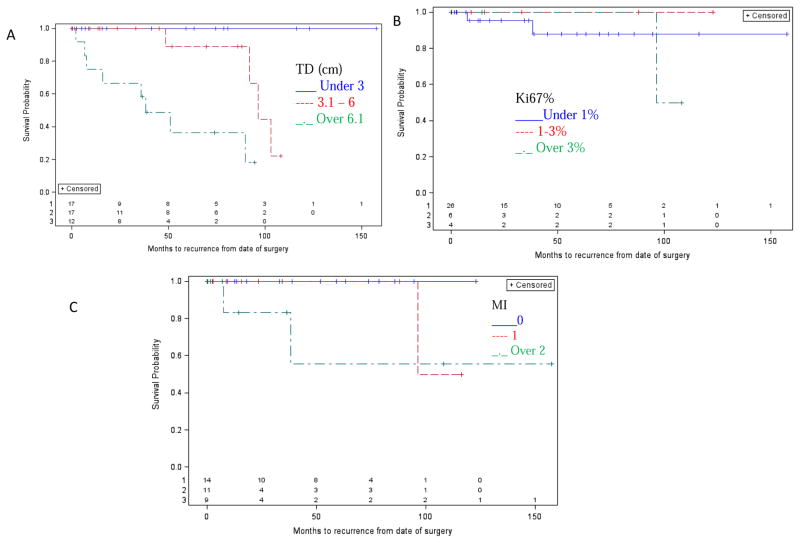
Results: Patients with SDHB mutation presented at younger age (33.0 years old vs 49.6 years old, P < .001), had increased local recurrence and distant metastases (47.6% vs 9.1%, P < .001, and 56.3% vs 9.1%, P < .001, respectively), and lesser median disease-free interval (89.8 months, 95% confidence interval 36.0-96.4 vs not reached, P < .001). SDHB mutation, greatest tumor diameter, and open operative resection were associated with a greater rate of local recurrence and distant metastases (P < .006 each). SDHB mutation and tumor diameter were independent risk factors for local recurrence (P ≤ .04 each) and metastases. Ki67% and mitotic index were not associated with SDHB mutation (P ≥ .09 each), local recurrence (P = .48, P = .066, respectively), metastases (P ≥ .22 each), or disease-free interval (P ≥ .19 each).
Conclusion: SDHB status and primary tumor size are more predictive of patient outcome than Ki67% or mitotic index and should be part of any clinically relevant, prognostic scoring system.
Published by Elsevier Inc.
Conflict of interest statement
of Potential Conflicts of Interest: The authors have no conflicts of interest to disclose.
Figures
Comment in
-
Discussion.Surgery. 2017 Jan;161(1):237-239. doi: 10.1016/j.surg.2016.05.054. Epub 2016 Nov 10. Surgery. 2017. PMID: 27839937 No abstract available.
References
-
- Zarnegar R, Kebebew E, Duh QY, Clark OH. Malignant pheochromocytoma. Surg Oncol Clin N Am. 2006;15:555–71. - PubMed
-
- Kebebew E, Duh QY. Benign and malignant pheochromocytoma: diagnosis, treatment, and follow-Up. Surg Oncol Clin N Am. 1998;7:765–89. - PubMed
-
- Rodriguez JM, Balsalobre M, Ponce JL, et al. Pheochromocytoma in MEN 2A syndrome. Study of 54 patients. World J Surg. 2008;32:2520–6. - PubMed
-
- Friedrich CA. Von Hippel-Lindau syndrome. A pleomorphic condition. Cancer. 1999;86:2478–82. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
