

Effectiveness of the EMPOWER-PAR Intervention in Improving Clinical Outcomes of Type 2 Diabetes Mellitus in Primary Care: A Pragmatic Cluster Randomised Controlled Trial
- PMID: 27842495
- PMCID: PMC5109682
- DOI: 10.1186/s12875-016-0557-1
Effectiveness of the EMPOWER-PAR Intervention in Improving Clinical Outcomes of Type 2 Diabetes Mellitus in Primary Care: A Pragmatic Cluster Randomised Controlled Trial
Abstract
Background: The chronic care model was proven effective in improving clinical outcomes of diabetes in developed countries. However, evidence in developing countries is scarce. The objective of this study was to evaluate the effectiveness of EMPOWER-PAR intervention (based on the chronic care model) in improving clinical outcomes for type 2 diabetes mellitus using readily available resources in the Malaysian public primary care setting.
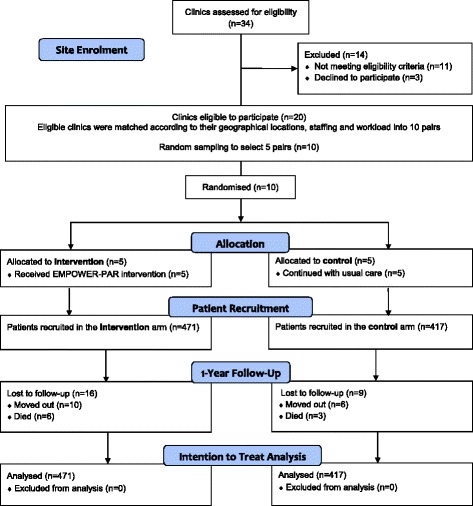
Methods: This was a pragmatic, cluster-randomised, parallel, matched pair, controlled trial using participatory action research approach, conducted in 10 public primary care clinics in Malaysia. Five clinics were randomly selected to provide the EMPOWER-PAR intervention for 1 year and another five clinics continued with usual care. Patients who fulfilled the criteria were recruited over a 2-week period by each clinic. The obligatory intervention components were designed based on four elements of the chronic care model i.e. healthcare organisation, delivery system design, self-management support and decision support. The primary outcome was the change in the proportion of patients achieving HbA1c < 6.5%. Secondary outcomes were the change in proportion of patients achieving targets for blood pressure, lipid profile, body mass index and waist circumference. Intention to treat analysis was performed for all outcome measures. A generalised estimating equation method was used to account for baseline differences and clustering effect.
Results: A total of 888 type 2 diabetes mellitus patients were recruited at baseline (intervention: 471 vs.
Control: 417). At 1-year, 96.6 and 97.8% of patients in the intervention and control groups completed the study, respectively. The baseline demographic and clinical characteristics of both groups were comparable. The change in the proportion of patients achieving HbA1c target was significantly higher in the intervention compared to the control group (intervention: 3.0% vs.
Control: -4.1%, P < 0.002). Patients who received the EMPOWER-PAR intervention were twice more likely to achieve HbA1c target compared to those in the control group (adjusted OR 2.16, 95% CI 1.34-3.50, P < 0.002). However, there was no significant improvement found in the secondary outcomes.
Conclusions: This study demonstrates that the EMPOWER-PAR intervention was effective in improving the primary outcome for type 2 diabetes in the Malaysian public primary care setting.
Trial registration: Registered with: ClinicalTrials.gov.: NCT01545401 . Date of registration: 1st March 2012.
Keywords: Chronic care model; Chronic disease management; Clinical outcomes; Family medicine; Multifaceted intervention; Primary care; Type 2 diabetes mellitus.
Figures

References
-
- International Diabetes Federation . IDF Diabetes Atlas. 7. Brussels: International Diabetes Federation; 2015. - PubMed
-
- World Health Organization. World Health Statistics [online]. Geneva: World Health Organization; 2014. [http://apps.who.int/iris/bitstream/10665/112738/1/9789240692671_eng.pdf].
-
- Institute for Public Health, Ministry of Health, Malaysia . National Health and Morbidity Survey 2011 (NHMS 2011) vol II: Non-Communicable Disease. Kuala Lumpur: Institute for Public Health; 2011.
-
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2197–223. http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(12)61689-.... - PubMed
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–128. doi: 10.1016/S0140-6736(12)61728-0. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
