

Complementary role of cardiac CT in the assessment of aortic valve replacement dysfunction
- PMID: 27843568
- PMCID: PMC5093391
- DOI: 10.1136/openhrt-2016-000494
Complementary role of cardiac CT in the assessment of aortic valve replacement dysfunction
Abstract
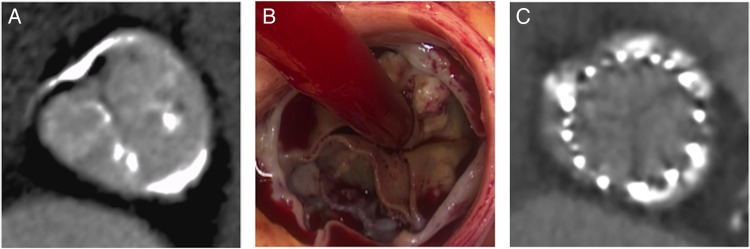
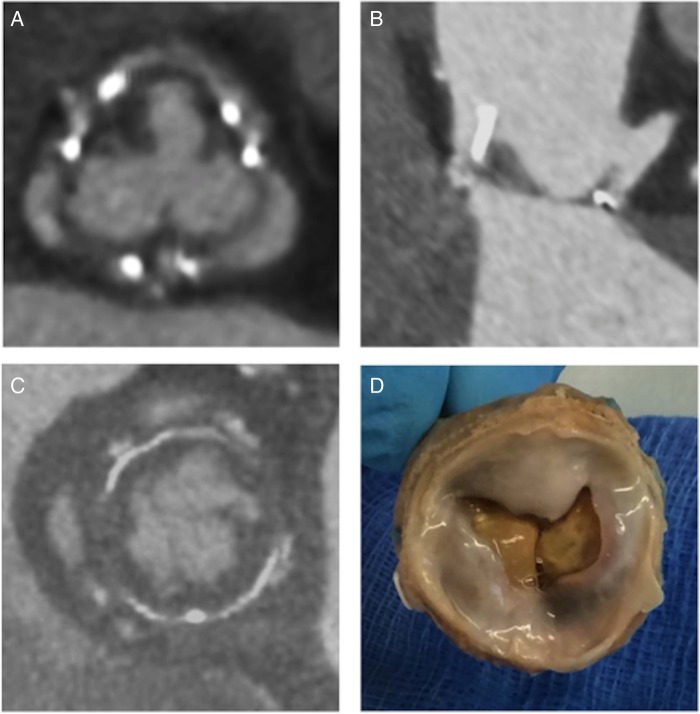
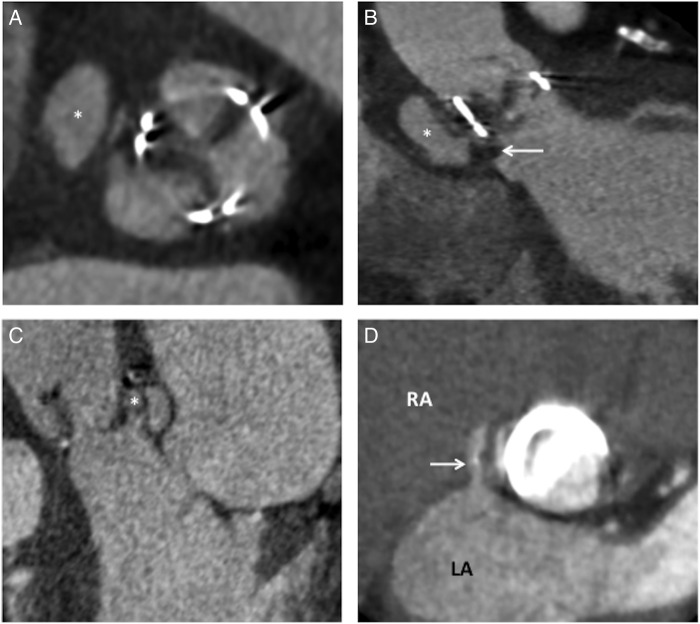
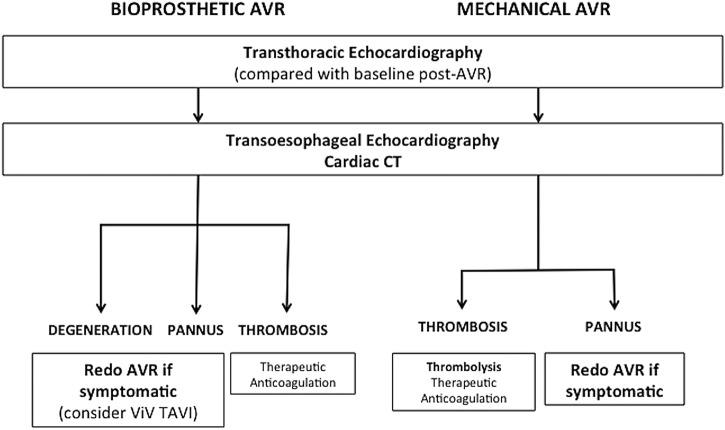
Aortic valve replacement is the second most common cardiothoracic procedure in the UK. With an ageing population, there are an increasing number of patients with prosthetic valves that require follow-up. Imaging of prosthetic valves is challenging with conventional echocardiographic techniques making early detection of valve dysfunction or complications difficult. CT has recently emerged as a complementary approach offering excellent spatial resolution and the ability to identify a range of aortic valve replacement complications including structural valve dysfunction, thrombus development, pannus formation and prosthetic valve infective endocarditis. This review discusses each and how CT might be incorporated into a multimodal cardiovascular imaging pathway for the assessment of aortic valve replacements and in guiding clinical management.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources