

Treatment and imaging of intracranial atherosclerotic stenosis: current perspectives and future directions
- PMID: 27843693
- PMCID: PMC5102638
- DOI: 10.1002/brb3.536
Treatment and imaging of intracranial atherosclerotic stenosis: current perspectives and future directions
Abstract
Background and purpose: Intracranial atherosclerosis is a common cause of stroke worldwide. It results in ischemic stroke due to different mechanisms including artery-to-artery embolism, in situ thrombo-occlusion, occlusion of perforating arteries, and hemodynamic failure. In this review, we present an overview of current treatment and imaging modalities in intracranial atherosclerotic stenosis.
Methods: PubMed was searched for relevant articles in English that evaluated the treatment and imaging of intracranial atherosclerotic stenosis (ICAS).
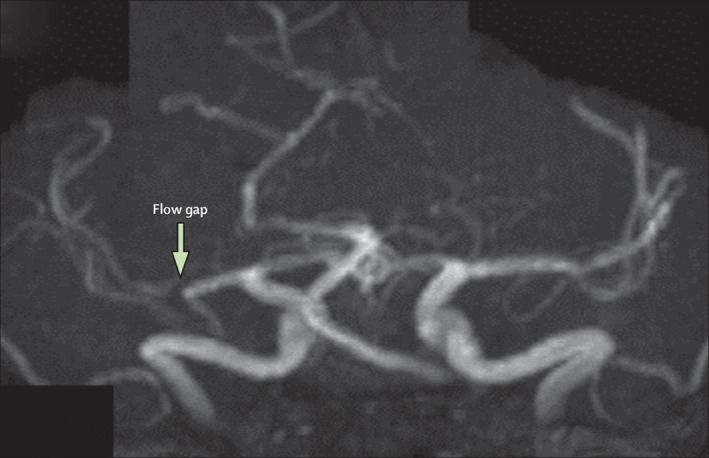
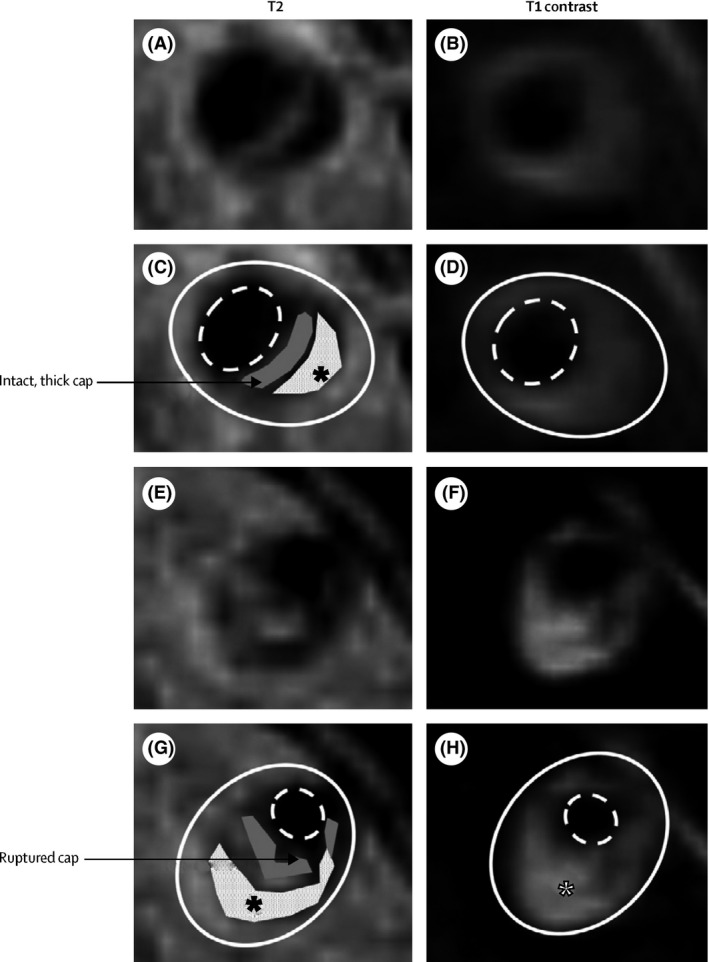
Results: Aggressive medical management, consisting of dual antiplatelet therapy and intensive risk factor management, is important in patients with ICAS because of a substantial risk of recurrent stroke, approximately 20% in the first year, in patients on aspirin or warfarin alone. Recent trials have suggested that, aggressive medical therapy results in better outcome as compared with intracranial stenting. However, the question remains what the optimal treatment strategy would be in patients with recurrent strokes in the setting of failed aggressive medical therapy. Moreover, controversy exists whether a subgroup of patients with symptomatic ICAS could benefit from intracranial stenting if selection is based on radiological evidence of hemodynamic failure. With regard to imaging, transcranial Doppler ultrasound and magnetic resonance angiography are useful screening tests for exclusion of ICAS, but need confirmation by other imaging modalities when stenosis is suggested. Computed tomography angiography has a high positive and negative predictive value for detection of intracranial luminal stenosis of 50% or higher, but performs worse than digital subtraction angiography with regard to establishing the exact degree of luminal stenosis. Novel imaging techniques including high-resolution CT and MRI better identify plaque characteristics than conventional imaging methods.
Conclusions: Currently, aggressive medical management remains the standard of care for patients with ICAS. Further research is needed to identify high-risk subgroups and to develop more effective treatments for ICAS patients.
Keywords: intracranial atherosclerosis; intracranial stenosis; ischemic stroke.
Figures

References
-
- Abou‐Chebl, A. , & Steinmetz, H. (2012). Critique of “Stenting versus aggressive medical therapy for intracranial arterial stenosis” by Chimowitz et al in the new England Journal of Medicine. Stroke, 43, 616–620. - PubMed
-
- Alexandrov, A. V. , Demchuk, A. M. , Wein, T. H. , & Grotta, J. C. (1999). Yield of transcranial Doppler in acute cerebral ischemia. Stroke, 30, 1604–1609. - PubMed
-
- Arenillas, J. F. (2011). Intracranial atherosclerosis: current concepts. Stroke, 42(1 Suppl), S20–S23. - PubMed
-
- Bash, S. , Villablanca, J. P. , Jahan, R. , Duckwiler, G. , Tillis, M. , Kidwell, C. , … Sayre, J. (2005). Intracranial vascular stenosis and occlusive disease: evaluation with CT angiography, MR angiography, and digital subtraction angiography. AJNR. American Journal of Neuroradiology, 26, 1012–1021. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
