

Rosacea Management
- PMID: 27843919
- PMCID: PMC5096126
- DOI: 10.1159/000446215
Rosacea Management
Abstract
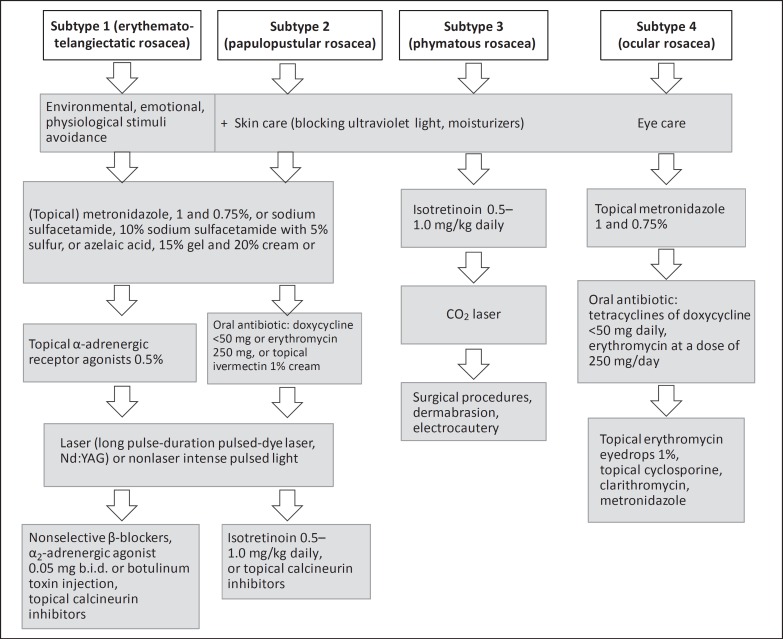
Background: Rosacea is a chronic inflammatory skin condition associated with four distinct subtypes: erythematotelangiectatic, papulopustular, phymatous, and ocular.
Purpose: To review the different kinds of management for all subtypes.
Methods: We divided rosacea management into three main categories: patient education, skin care, and pharmacological/procedural interventions.
Results: Flushing is better prevented rather than treated, by avoiding specific triggers, decreasing transepidermal water loss by moisturizers, and blocking ultraviolet light. Nonselective β-blockers and α2-adrenergic agonists decrease erythema and flushing. The topical α-adrenergic receptor agonist brimonidine tartrate 0.5% reduces persistent facial erythema. Intradermal botulinum toxin injection is almost safe and effective for the erythema and flushing. Flashlamp-pumped dye, potassium-titanyl-phosphate and pulsed-dye laser, and intense pulsed light are used for telangiectasias. Metronidazole 1% and azelaic acid 15% cream reduce the severity of erythema. Both systemic and topical remedies treat papulopustules. Systemic remedies include metronidazole, doxycycline, minocycline, clarithromycin and isotretinoin, while topical remedies are based on metronidazole 0.75%, azelaic acid 15 or 20%, sodium sulfacetamide, ivermectin 1%, permethrin 5%, and retinoid. Ocular involvement can be treated with oral or topical antibacterial. Rhinophyma can be corrected by dermatosurgical procedures, decortication, and various types of lasers.
Conclusion: There are many options for rosacea management. Patients may have multiple subtypes, and each phase has its own treatment.
Keywords: Azelaic acid; Demodex; Inflammatory lesion; Isotretinoin; Ivermectin; Laser; Ocular rosacea; Rosacea.
References
-
- Gupta AK, Chaudhry MM. Rosacea and its management: an overview. J Eur Acad Dermatol Venereol. 2005;19:273–285. - PubMed
-
- National Rosacea Society http://www.rosacea.org/tags/rosacea-awareness-month. www.rosacea.org/patients/allaboutrosacea.php.
-
- Two AM, Wu W, Gallo RL, Hata TR. Topical and systemic therapies in the treatment of rosacea. J Am Acad Dermatol. 2015;72:761–770. quiz 771-772. - PubMed
-
- Rebora A. The management of rosacea. Am J Clin Dermatol. 2002;3:489–496. - PubMed
-
- Bernstein EF, Kligman A. Rosacea treatment using the new-generation, high-energy, 595 nm, long pulse-duration pulsed-dye laser. Lasers Surg Med. 2008;40:233–239. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
