

Granulocyte-Colony Stimulating Factor (G-CSF) for stroke: an individual patient data meta-analysis
- PMID: 27845349
- PMCID: PMC5109224
- DOI: 10.1038/srep36567
Granulocyte-Colony Stimulating Factor (G-CSF) for stroke: an individual patient data meta-analysis
Abstract
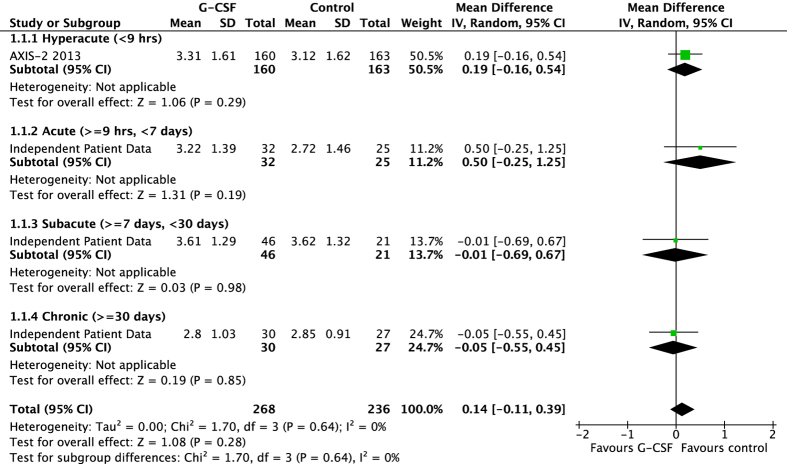
Granulocyte colony stimulating factor (G-CSF) may enhance recovery from stroke through neuroprotective mechanisms if administered early, or neurorepair if given later. Several small trials suggest administration is safe but effects on efficacy are unclear. We searched for randomised controlled trials (RCT) assessing G-CSF in patients with hyperacute, acute, subacute or chronic stroke, and asked Investigators to share individual patient data on baseline characteristics, stroke severity and type, end-of-trial modified Rankin Scale (mRS), Barthel Index, haematological parameters, serious adverse events and death. Multiple variable analyses were adjusted for age, sex, baseline severity and time-to-treatment. Individual patient data were obtained for 6 of 10 RCTs comprising 196 stroke patients (116 G-CSF, 80 placebo), mean age 67.1 (SD 12.9), 92% ischaemic, median NIHSS 10 (IQR 5-15), randomised 11 days (interquartile range IQR 4-238) post ictus; data from three commercial trials were not shared. G-CSF did not improve mRS (ordinal regression), odds ratio OR 1.12 (95% confidence interval 0.64 to 1.96, p = 0.62). There were more patients with a serious adverse event in the G-CSF group (29.6% versus 7.5%, p = 0.07) with no significant difference in all-cause mortality (G-CSF 11.2%, placebo 7.6%, p = 0.4). Overall, G-CSF did not improve stroke outcome in this individual patient data meta-analysis.
Figures
References
-
- Murray C. J. & Lopez A. D. Mortality by cause for eight regions of the world: Global Burden of Disease Study. Lancet 349, 1269–1276 (1997). - PubMed
-
- Dunac A. et al.. Neurological and functional recovery in human stroke are associated with peripheral blood CD34+ cell mobilization. J Neurol 254, 327–332 (2007). - PubMed
-
- Hennemann B. et al.. Mobilization of CD34+ hematopoietic cells, colony-forming cells and long-term culture-initiating cells into the peripheral blood of patients with an acute cerebral ischemic insult. Cytotherapy 10, 303–311 (2008). - PubMed
-
- Schabitz W. R. et al.. Neuroprotective effect of granulocyte colony-stimulating factor after focal cerebral ischemia. Stroke 34, 745–751 (2003). - PubMed
-
- Kollmar R., Henninger N., Urbanek C. & Schwab S. G-CSF and rt-PA for the treatment of experimental embolic stroke. Cerebrovascular Diseases 23, 23 (2007).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
