

Refractory pituitary adenoma: a novel classification for pituitary tumors
- PMID: 27845901
- PMCID: PMC5347795
- DOI: 10.18632/oncotarget.13274
Refractory pituitary adenoma: a novel classification for pituitary tumors
Abstract
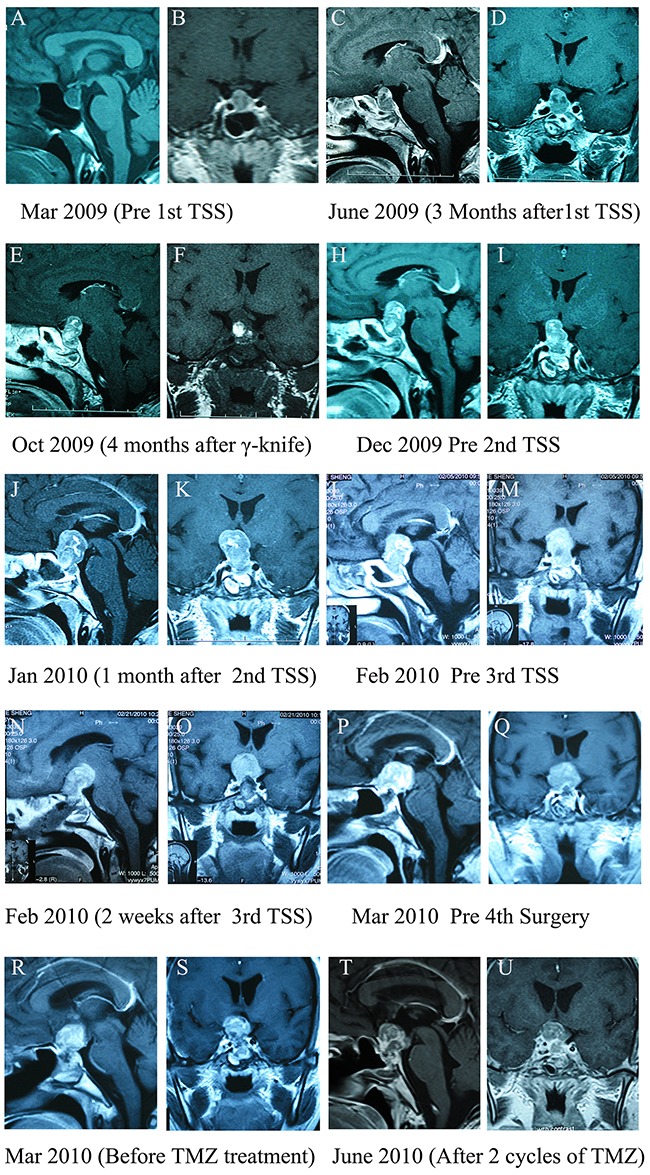
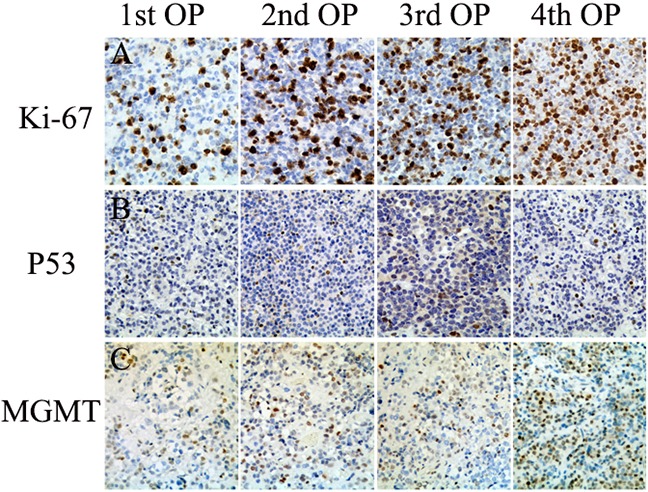
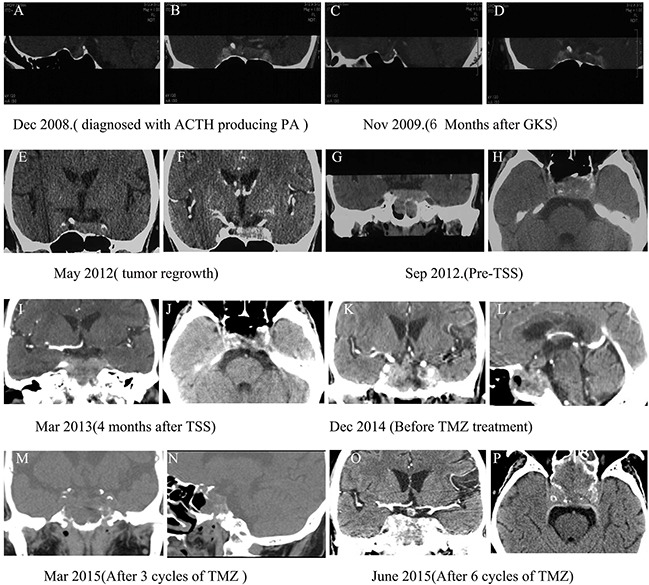
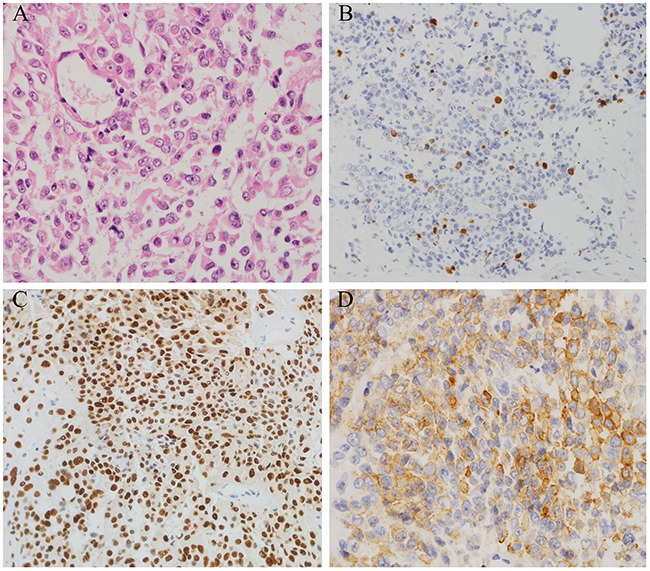
Pituitary adenomas are classified as typical or atypical, invasive or noninvasive, and aggressive or nonaggressive based on pathological features, radiological findings, and clinical behavior. Only pituitary tumors with cerebrospinal and/or systemic metastasis are considered malignant carcinomas. However, some pituitary adenomas with high Ki-67 indexes exhibit aggressive behaviors, such as rapid growth, early and frequent recurrence, and resistance to conventional treatment, even in the absence of metastasis. Novel terminology is needed to define these tumors. Here, we propose the use of the term "refractory pituitary adenoma" to define malignant pituitary tumors exhibiting 1) a high Ki-67 index and rapid growth, 2) early and high frequency of recurrence, 3) resistance to conventional treatments and/or salvage treatment with temozolomide (TMZ), 4) poor prognosis, 5) and a lack of cerebrospinal or systemic metastases. To illustrate the utility of this refractory pituitary adenoma classification and the difficulty in managing disease in these patients, we examined twelve clinical cases. Correctly identifying refractory pituitary adenomas is crucial for improving patient prognoses. Early identification might encourage the early use of aggressive therapeutic strategies to prevent or delay recurrence.
Keywords: aggressive; pituitary adenomas; recurrence; refractory; resistance.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Asa SL, Ezzat S. The cytogenesis and pathogenesis of pituitary adenomas. Endocr Rev. 1998;19:798–827. - PubMed
-
- Meij BP, Lopes MB, Ellegala DB, Alden TD, Laws EJ. The long-term significance of microscopic dural invasion in 354 patients with pituitary adenomas treated with transsphenoidal surgery. J Neurosurg. 2002;96:195–208. - PubMed
-
- Kontogeorgos G. Innovations and controversies in the WHO classification of pituitary adenomas. Acta Neuropathol. 2006;111:73–75. - PubMed
-
- Heaney A. Management of aggressive pituitary adenomas and pituitary carcinomas. J Neuro-Oncol. 2014;117:459–468. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
