

Systematic Review and Meta-Analysis of Randomised Trials to Ascertain Fatal Gastrointestinal Bleeding Events Attributable to Preventive Low-Dose Aspirin: No Evidence of Increased Risk
- PMID: 27846246
- PMCID: PMC5113022
- DOI: 10.1371/journal.pone.0166166
Systematic Review and Meta-Analysis of Randomised Trials to Ascertain Fatal Gastrointestinal Bleeding Events Attributable to Preventive Low-Dose Aspirin: No Evidence of Increased Risk
Abstract
Background: Aspirin has been shown to lower the incidence and the mortality of vascular disease and cancer but its wider adoption appears to be seriously impeded by concerns about gastrointestinal (GI) bleeding. Unlike heart attacks, stroke and cancer, GI bleeding is an acute event, usually followed by complete recovery. We propose therefore that a more appropriate evaluation of the risk-benefit balance would be based on fatal adverse events, rather than on the incidence of bleeding. We therefore present a literature search and meta-analysis to ascertain fatal events attributable to low-dose aspirin.
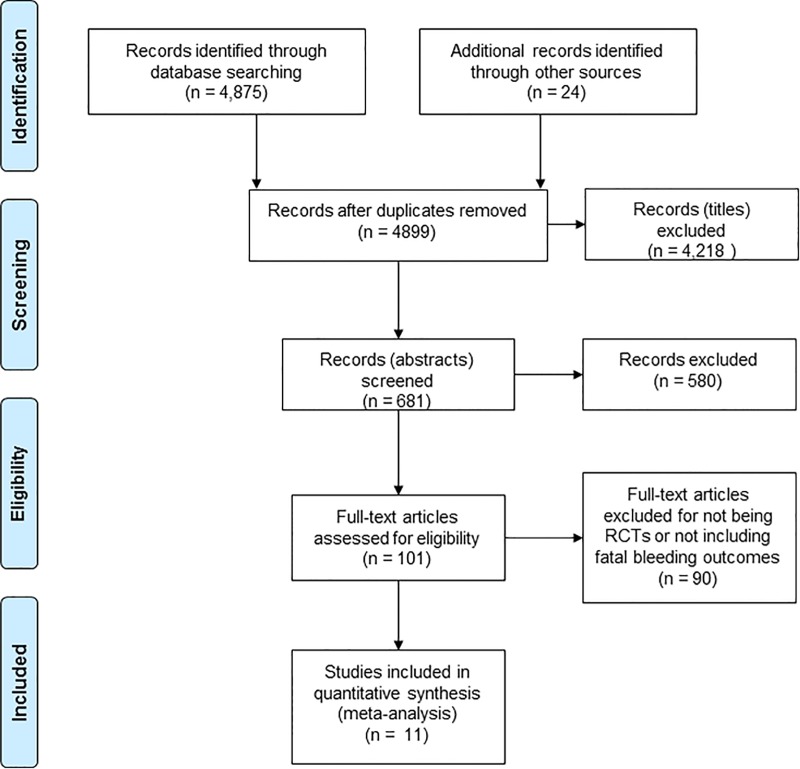
Methods: In a systematic literature review we identified reports of randomised controlled trials of aspirin in which both total GI bleeding events and bleeds that led to death had been reported. Principal investigators of studies in which fatal events had not been adequately described were contacted via email and asked for further details. A meta-analyses was then performed to estimate the risk of fatal gastrointestinal bleeding attributable to low-dose aspirin.
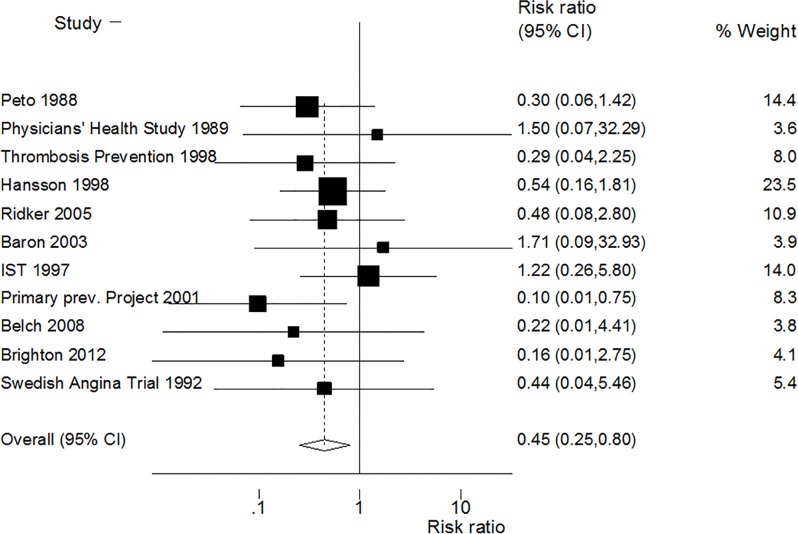
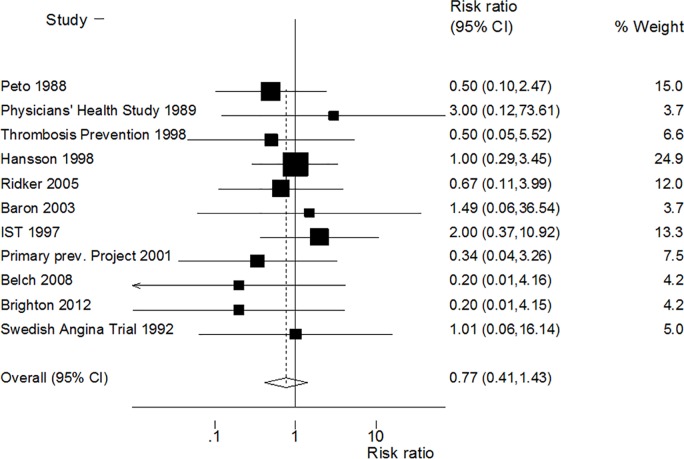
Results: Eleven randomised trials were identified in the literature search. In these the relative risk (RR) of 'major' incident GI bleeding in subjects who had been randomised to low-dose aspirin was 1.55 (95% CI 1.33, 1.83), and the risk of a bleed attributable to aspirin being fatal was 0.45 (95% CI 0.25, 0.80). In all the subjects randomised to aspirin, compared with those randomised not to receive aspirin, there was no significant increase in the risk of a fatal bleed (RR 0.77; 95% CI 0.41, 1.43).
Conclusions: The majority of the adverse events caused by aspirin are GI bleeds, and there appears to be no valid evidence that the overall frequency of fatal GI bleeds is increased by aspirin. The substantive risk for prophylactic aspirin is therefore cerebral haemorrhage which can be fatal or severely disabling, with an estimated risk of one death and one disabling stroke for every 1,000 people taking aspirin for ten years. These adverse effects of aspirin should be weighed against the reductions in vascular disease and cancer.
Conflict of interest statement
We have the following conflicts: PCE was an advisor to Bayer HealthCare and was until recently a member of the Board of the International Aspirin Foundation. JMG is a consultant to Bayer and the Chair of the executive committee for the ARRIVE trial which is sponsored by Bayer. AL has participated in Advisory Boards organized by Bayer Pharma AG. JWKC has previously participated in Advisory Boards by Bayer AG. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Age-specific risks, severity, time course, and outcome of bleeding on long-term antiplatelet treatment after vascular events: a population-based cohort study.Lancet. 2017 Jul 29;390(10093):490-499. doi: 10.1016/S0140-6736(17)30770-5. Epub 2017 Jun 13. Lancet. 2017. PMID: 28622955 Free PMC article.
-
Major GI bleeding in older persons using aspirin: incidence and risk factors in the ASPREE randomised controlled trial.Gut. 2021 Apr;70(4):717-724. doi: 10.1136/gutjnl-2020-321585. Epub 2020 Aug 3. Gut. 2021. PMID: 32747412 Free PMC article. Clinical Trial.
-
Benefits and Risks Associated with Low-Dose Aspirin Use for the Primary Prevention of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Randomized Control Trials and Trial Sequential Analysis.Am J Cardiovasc Drugs. 2022 Nov;22(6):657-675. doi: 10.1007/s40256-022-00537-6. Epub 2022 May 16. Am J Cardiovasc Drugs. 2022. PMID: 35570250
-
Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials.Lancet. 2009 May 30;373(9678):1849-60. doi: 10.1016/S0140-6736(09)60503-1. Lancet. 2009. PMID: 19482214 Free PMC article.
-
A comparison of contemporary versus older studies of aspirin for primary prevention.Fam Pract. 2020 Jul 23;37(3):290-296. doi: 10.1093/fampra/cmz080. Fam Pract. 2020. PMID: 31751455
Cited by
-
Aspirin and cancer treatment: systematic reviews and meta-analyses of evidence: for and against.Br J Cancer. 2024 Jan;130(1):3-8. doi: 10.1038/s41416-023-02506-5. Epub 2023 Nov 29. Br J Cancer. 2024. PMID: 38030748 Free PMC article.
-
Low-dose aspirin and risk of upper/lower gastrointestinal bleeding by bleed severity: a cohort study with nested case-control analysis using primary care electronic health records from the United Kingdom.Ann Med. 2019 Mar;51(2):182-192. doi: 10.1080/07853890.2019.1591635. Epub 2019 Apr 26. Ann Med. 2019. PMID: 31025592 Free PMC article.
-
Beneficial Prognostic Effects of Aspirin in Patients Receiving Sorafenib for Hepatocellular Carcinoma: A Tale of Multiple Confounders.Cancers (Basel). 2021 Dec 20;13(24):6376. doi: 10.3390/cancers13246376. Cancers (Basel). 2021. PMID: 34944996 Free PMC article.
-
Mortality among patients due to adverse drug reactions that lead to hospitalization: a meta-analysis.Eur J Clin Pharmacol. 2018 Jun;74(6):819-832. doi: 10.1007/s00228-018-2441-5. Epub 2018 Mar 19. Eur J Clin Pharmacol. 2018. PMID: 29556685
-
Postdiagnosis Aspirin Use Associated With Decreased Biliary Tract Cancer-Specific Mortality in a Large Nationwide Cohort.Hepatology. 2021 Oct;74(4):1994-2006. doi: 10.1002/hep.31879. Epub 2021 Jul 20. Hepatology. 2021. PMID: 33942350 Free PMC article.
References
-
- American Cancer Society and Livestrong Report. The Global Economic Impact of Cancer. http://www.cancer.org/acs/grpups/conmtent@internationalaffairs/documents....
-
- Bloom DE, Cafiero ET., Jané-Llopis E, Abrahams-Gessel S, Bloom LR, Fathima S. et al. The Global Economic Burden of noncommunicable diseases World Economic Forum.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
